
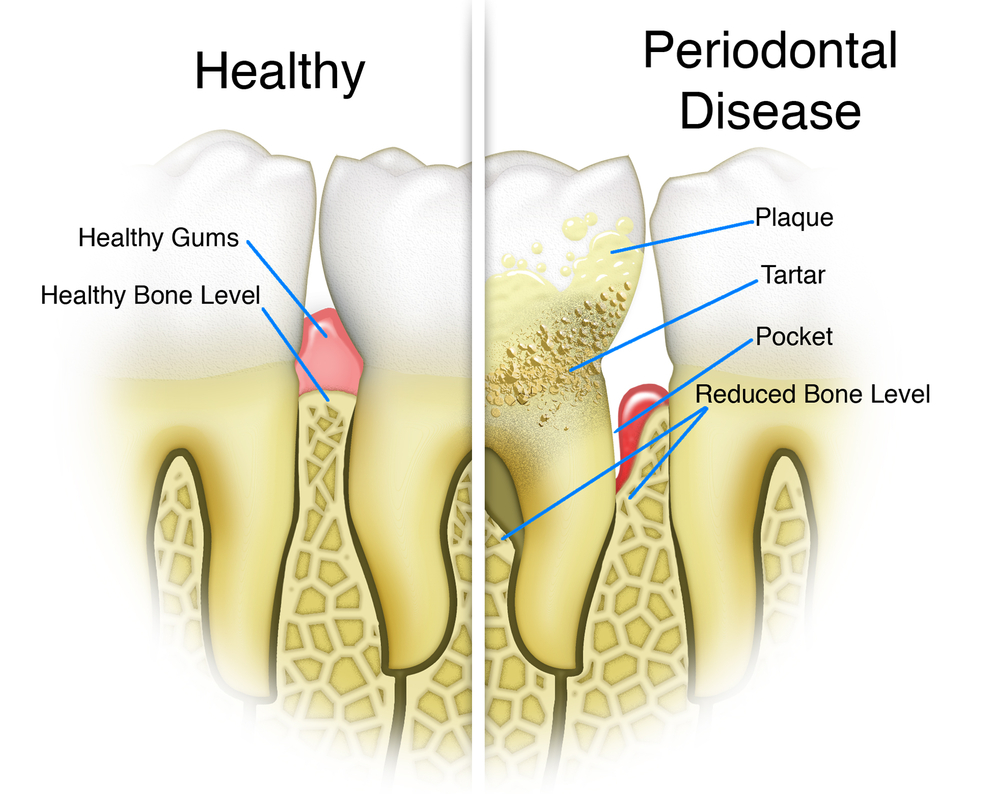
Periodontal disease lead to loss of connective tissue attachment and loss of alveolar bone supporting the teeth. Two patterns of bone destruction are described suprabony (horizontal) defects and infrabony (vertical) defects. Left untreated these bony defects help promote progression of periodontitis. A number of surgical approaches are available for the treatment of periodontitis and recently autologous platelet concentrates (APC) have been used as an adjunct with the view to promoting healing.
The aim of this Cochrane review was to assess the effects of autologous platelet concentrates (APC) used as an adjunct to periodontal surgical therapies (open flap debridement (OFD), OFD combined with bone grafting (BG), guided tissue regeneration (GTR), OFD combined with enamel matrix derivative (EMD)) for the treatment of infrabony defects.
Methods
Searches were conducted in the Cochrane Oral Health’s Trials Register, Cochrane Central Register of Controlled Trials (CENTRAL), Medline, Embase, LILACS BIREME Virtual Health Library, The US National Institutes of Health Ongoing Trials Register (ClinicalTrials.gov) and the World Health Organization International Clinical Trials Registry Platform with no restrictions on date or language. Parallel and split-mouth randomised controlled trials (RCTs) in patients with infrabony defects requiring surgical treatment that compared a specific surgical technique combined with APC against the same technique alone were considered.
Two review authors independently selected studies, extracted data and conducted a risk of bias assessment. Data analysis followed standard Cochrane methodology. The primary outcomes were change in probing pocket depth (PD), change in clinical attachment level (CAL), and change in radiographic bone defect filling (RBF).
Results
- 38 RCTs (22 split-mouth, 16 parallel) evaluating 1402 defects were included.
- 36 RCTs were at high risk of bias and 2 were at unclear risk.
- APC + OFD versus OFD alone
- Twelve studies were included in this comparison, with a total of 510 infrabony defects.
- There is very low-quality evidence of an advantage in using APC globally from split-mouth and parallel studies for all three primary outcomes.
- APC + OFD + BG versus OFD + BG
- Seventeen studies were included in this comparison, with a total of 569 infrabony defects.
- Considering all follow-ups, as well as 3 to 6 months and 9 to 12 months, there is very low-quality evidence of an advantage in using APC from both split-mouth and parallel studies for all three primary outcomes:
- APC + GTR versus GTR alone
- Seven studies were included in this comparison, with a total of 248 infrabony defects.
- Considering all follow-ups, there is probably a benefit for APC for both PD) and CAL. However, given the wide confidence intervals, there might be a possibility of a slight benefit for the control. When considering a 3 to 6 months and a 9 to 12 months follow-up there were no benefits evidenced, except for CAL at 3 to 6 months (MD 0.54 mm, 95% CI 0.18 to 0.89 mm; P = 0.003; 3 studies; 134 defects). No RBF data were available.
- APC + EMD versus EMD
- Two studies were included in this comparison, with a total of 75 infrabony defects.
- There is insufficient evidence of an overall advantage of using APC for all three primary outcomes:
- All studies in all groups reported a survival rate of 100% for the treated teeth. No complete pocket closure was reported. No quantitative analysis regarding patients’ quality of life was possible.
| Intervention | No. Studies (defects) | PD
MD (95%CI) |
CAL
MD (95%CI) |
RBF *
MD ( 95%CI) |
| APC + OFD versus OFD alone | 12 (510) | 1.29 mm (1.00 to 1.58 mm) | 1.47 mm (1.11 to 1.82 mm) | 34.26% (30.07% to 38.46%) |
| APC + OFD + BG versus OFD + BG | 17 (569) | 0.54 mm (0.33 to 0.75 mm) | 0.72 mm (0.43 to 1.00 mm) | 8.10% (5.26% to 10.94%) |
| APC + GTR versus GTR alone | 7 (248) | 0.92 mm (0.02 to 1.86 mm) | 0.42 mm(-0.02 to 0.86 mm | N/A |
| APC + EMD versus EMD | 2 (75) | 0.13 mm (-0.05 to 0.30 mm) | 0.10 mm(-0.13 to 0.32 mm) | -0.60% (-6.21% to 5.01%) |
MD= Mean difference
* For each intervention the number of studies and defects providing information was fewer than for PD and CAL.
Conclusions
The authors concluded: –
There is very low-quality evidence that the adjunct of APC to OFD or OFD + BG when treating infrabony defects may improve probing pocket depth, clinical attachment level, and radiographic bone defect filling. For GTR or EMD, insufficient evidence of an advantage in using APC was observed.
Comments
The use of APCs is a relatively adjunct to periodontal surgery with most of the studies including in this review having taken place in the last decade. Autologous platelet concentrates can be divided into four categories, based on the presence of leucocyte and fibrin: P-PRP (pure PRP, without leucocytes, which includes PRGF), L-PRP (leucocyte and platelet-rich plasma), P-PRF (pure PRF), and L-PRF (leucocyte PRF). The range of APCs available and the different periodontal surgical procedure provide a wide range of potential variation. This means that despite that fact that 38 trials were identified for this review there are a limited number of studies for each approach. This is compounded by the small size of the studies and the high risk of bias for almost all the studies. The main reason for assigning high risk of bias is related to the blinding of patients and study personnel. So while the review found very low-quality evidence that adjunctive APC with open flap debridement and open flap debridement with bone graft further high quality studies are needed.
Links
Primary Paper
Del Fabbro M, Karanxha L, Panda S, Bucchi C, Nadathur Doraiswamy J, Sankari M, Ramamoorthi S, Varghese S, Taschieri S. Autologous platelet concentrates for treating periodontal infrabony defects.
Cochrane Database of Systematic Reviews 2018, Issue 11. Art. No.: CD011423.
DOI: 10.1002/14651858.CD011423.pub2.
Other references


