

[Note: today’s blog is very much a group effort. It’s been written by more than 20 MSc students at University College London who had an elf (yours truly) gatecrash their journal club on Wednesday! Do let me know if you want me to infiltrate your journal club. We elves have our ways you know.]
Previous research has found associations between trauma and psychotic symptoms. However, the search for causality continues. According to the Bradford Hill criteria, several requirements must be fulfilled in order to establish causality.
We already know from past evidence that associations between trauma and psychosis have been robustly replicated with evidence of a clear dose-response relationship (Varese et al, 2012; van Dam, 2012). Evidence also suggests that a temporal sequence exists between trauma and psychosis and that resolving trauma reduces psychotic symptoms.
However, studies have not fulfilled a remaining criterion; that plausible theory-based mechanisms explain the associations between trauma and psychosis. This new study (Hardy et al, 2016) aims to address this gap in our knowledge.
This study had two aims.
- The first was to replicate the previously established association between trauma and psychotic symptoms
- The second was to test their theory-based hypotheses about potential causal mechanisms.
To test the first aim, the authors hypothesised that childhood sexual abuse would be associated with auditory hallucinations, and that childhood physical abuse would be associated with paranoia.
To test the second aim, they proposed four hypotheses:
- Intrusive trauma memories were hypothesised to mediate the association between childhood sexual abuse and hallucinations
- They hypothesised that negative beliefs about the self and others mediated the association between childhood physical abuse and paranoia
- Trauma-related affect regulation (numbing, avoidance and hyperarousal) was hypothesised to mediate the relationship between all trauma types and all psychotic symptoms
- They also proposed that depression mediates the relationship between all trauma types and all psychotic symptoms.

Methods
228 participants were recruited from 4 NHS trusts in London and East Anglia, via a UK randomised controlled trial of CBT and family intervention for psychosis.
Inclusion criteria
- Aged 18-65
- Recent relapse in positive symptoms
- Diagnosis of non-affective psychosis
- Score of 4 of the Positive and Negative Syndrome scale (PANSS).
Exclusion criteria
- Primary diagnosis of a substance misuse, learning disability, or organic syndrome
- Insufficient level of English.
Measures
Cross-sectional design, included five measures:
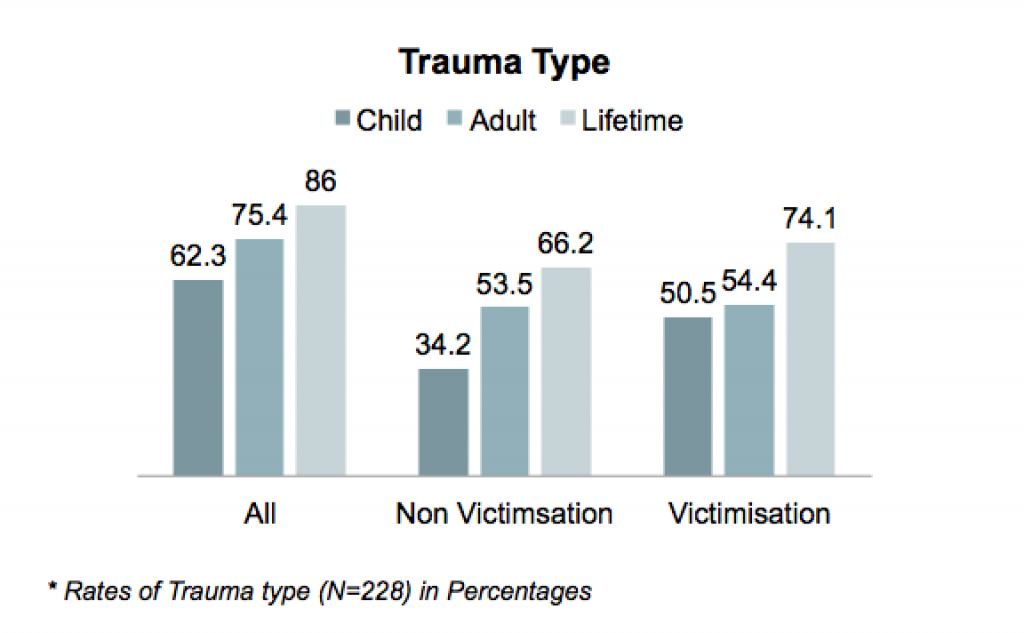
The Trauma History Questionnaire (THQ)
- An assessment of:
- Non-victimisation: Illness, natural disasters, accidents
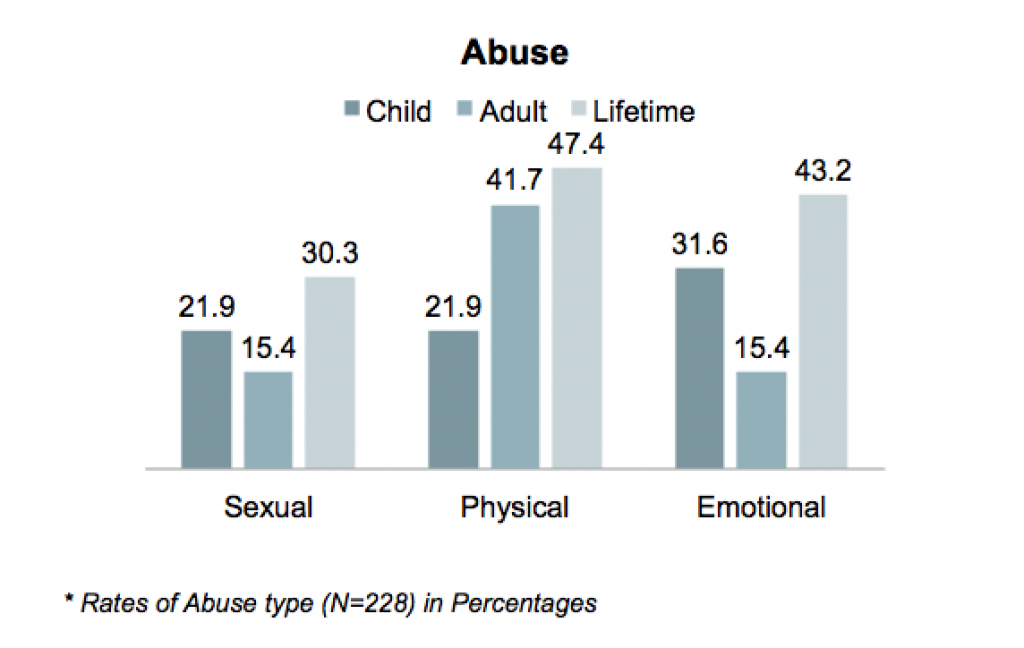
- Victimisation: Sexual abuse, Physical abuse and Emotional abuse
- If participants reported at least 1 event, they were asked to indicate which trauma they were currently most affected by as their ‘index event’
- All reported events were categorised into childhood, adulthood, or lifetime
Post-traumatic Stress Disorder (SRS- PTSD): This looked at PTSD symptoms in relation to the event that the participants reported they were most affected by.
The Scales for the Assessment of Positive Symptoms: Looking at positive symptoms of psychosis over the past month
The Brief Core Schema Scale (BCSS): To assess the core beliefs; either on the self-belief or negative-other scales
The Beck Depression Inventory (BDI-II): Depression is assessed over the past fortnight.
Analysis
The analyses were carried out in 3 stages:
- Associations between all trauma types and symptoms of psychosis
- Those associations that were found to be significant were then assessed to look at the total effect of trauma exposure on symptoms of psychosis
- Effect of trauma exposure on the mediators, using a linear regression
- Both of these stages adjusted for age, gender, and ethnicity as potential confounders
- Only those trauma-outcome and trauma-mediator relationships which were statistically significant at the 10% level were carried forward into the mediation analysis
- Mediation analysis was then done to test whether a proposed mechanism can explain the association between trauma and psychosis
- A framework was used at this stage, and it allowed for the estimate of the Natural Direct Effects (NDE) and Natural Indirect Effects (NIE).
If the NIE pathway was statistically significant, this would reflect a partial indirect effect of the mediator. However, if the NDE pathway was also found to be non-significant, then this would be considered evidence of full mediation.
Results
- The authors of the study divided the rates of trauma and abuse, on the different prevalent rates, based upon the participant response on the Trauma History Questionnaire (THQ):
- The researchers found a statistically significant association between child sexual abuse with auditory hallucinations (OR = 3, CI = 1.2 to 4.3, P = 0.12)
- They did not find a statistically significant association between child physical abuse and paranoia (OR = 1.2, CI = 0.6 to 2.3, P = 0.555)
- Interestingly, going beyond the scope of the hypothesis in the study, the authors found a statistically significant association between child emotional abuse and persecutory beliefs (OR = 1.9, CI = 1.1 to 3.5, P = 0.022) and delusions of reference (OR = 2.1, CI = 1.2 to 3.8, P=0.009)
- The study found an indirect effect of cognitive-affective factors of post-traumatic avoidance, numbing (OR = 1.475, SE = 188, P = 0.038) and hyper-arousal (OR = 1.439, SE = 0.184, P = 0.048) on the development of auditory hallucinations when someone is exposed to child sexual abuse
- Further, the study found similar indirect effect of negative other beliefs on the development of delusions of persecution when an individual was exposed to child emotional abuse (OR = 1.359, SE = 0.136, P = 0.024).

Conclusions
The authors concluded:
This study is the first to demonstrate that trauma-related psychological mechanisms mediate victimization and psychotic symptoms associations in a large sample of people with relapsing psychosis.
The identification of theoretically based psychological processes underlying specific associations between events and symptoms provides further support for the causal role of trauma in psychosis.
This the first evidence for theory in the relationship between trauma and subsequent psychosis is particularly interesting because they found that the mediators depended on the different types of trauma (emotional, sexual, physical). The authors concluded that these trauma-specific mechanisms could suggest a new direction for practice in the near future; providing tailored treatments for different types of victimisation.
It certainly does seem to resonate with growing prophecies of an age of personalised medicine, but we aren’t quite there yet. Translating research into practice is a long process, and requires lots of high quality research. Which begs the question: how did this study fare in the critical review of keen eyed MSc students?
Strengths and limitations
One particularly important aspect of this study is that it was the first of it’s kind (while previous studies had investigated the link between trauma and psychosis, no past research had looked at what variables mediated this relationship); nobody had looked at why the relationship occurred. The study was also novel in terms of exploring links between specific types of trauma and specific psychotic symptoms. Acknowledging the variation of different trauma types and different symptoms is of great importance for both research and clinical practice.
Although the importance of investigating mediators of the trauma/psychosis relationship is undeniable, there are difficulties with accepting the conclusions about these mediators, given the methodology used in the study. A cross sectional design was used, meaning that data collection for all variables happened at the same time. Accounts of trauma were therefore retrospective. This creates several issues:
- Individuals might be more likely to have selectively reported more recent trauma
- Subsequent experience of treatment might affect retrospective reports of trauma if individuals are exploring past events in therapy
- But mainly, we don’t know that a variable is a mediator unless we know that it occurred before the outcome and in this study, we can’t make this assumption.
One way to test this would be to measure trauma and mediators first and then measure outcome at some later stage, in other words, to use a prospective cohort or longitudinal study design. But this kind of design comes with its own demands, requiring a larger sample, considerable ethical consideration, more time and money. Finding some compromise between this and the design the author’s used might be the best option for investigating this area further.
Another issue that may need to be improved upon in further research is how trauma events are categorised. In this study, a given trauma event was categorised by researchers as either childhood emotional, physical or sexual abuse. There was no consideration for trauma events that may have fallen into more than one category, but if sexual abuse is experienced, surely this could be experienced as emotional abuse as well? This categorisation undermines the results because it means that accurate measurement of trauma types is not guaranteed. Also, inclusion of other specific trauma types would have been useful. Neglect, for example, which has been linked with psychosis in males in particular, is not included as a trauma category.

Implications
Seeing as this was a study in a novel area, the evidence regarding the mechanisms leading to psychosis is still very tentative; however, Hardy et al.’s (2016) research does prompt interesting questions. Considering the evidence discussed, our questions regarding implications of this research are three fold.
- Firstly, does this suggest interventions such as CBT should be used to target specific psychological mechanism? For example, if research shows that negative self-belief mediates the relationship between childhood sexual abuse and auditory hallucinations, should we target this?
- Secondly, should professionals who work directly with service users be looking into a service users history for signs of trauma? As a service user, is this something that you would find helpful, or would it be more like opening a can of worms?
- Finally, there has been a lot of caution around using psychodynamic approaches in the treatment of psychosis. But might asking the service user to look back into their own history highlight potential mechanisms?

Links
Primary paper
Hardy A, Emsley R, Freeman D, Bebbington P, Garety PA, Kuipers EE, Dunn G, Fowler D. (2016) Psychological Mechanisms Mediating Effects Between Trauma and Psychotic Symptoms: The Role of Affect Regulation, Intrusive Trauma Memory, Beliefs, and Depression. Schizophr Bull (2016) 42 (suppl 1): S34-S43 doi:10.1093/schbul/sbv175
Other references
Varese F, Smeets F, Drukker M, Lieverse R, Lataster T, Viechtbauer W, Read J, van Os J, Bentall RP. (2012) Childhood adversities increase the risk of psychosis: a meta-analysis of patient-control, prospective- and cross-sectional cohort studies. Schizophr Bull. 2012;38:661–671.
van Dam DS, van der Ven E, Velthorst E, Selten JP, Morgan C, de Haan L. (2012) Childhood bullying and the association with psychosis in non-clinical and clinical samples: a review and meta-analysis. Psychol Med. 2012;42:2463–2474. [PubMed abstract]




Trauma-informed approaches in mental health: co-optable & corruptible?
7 years agoWhat happened to you? Trauma informed approaches to mental health
8 years agoRichard Bentall
8 years agoAmy Hardy
9 years agoDuallaOne
9 years agoerinisaway
9 years agoArianeBeeston
9 years agoabbasian
9 years agoAdibEssali
9 years agoEuro_Psychiatry
9 years agoKentSmalley
9 years agoYasTheLaz
9 years agoborromeannot
9 years agoHowardNWhite
9 years agoIABCP_CBT
9 years agoBABCP
9 years agovalidconsent
9 years agoSameiHuda
9 years agoMariaLourenzo
9 years agoTimothyBrow
9 years agorosj14
9 years agoMentalhealthMSc
9 years agoPaulineWatts10
9 years agoMental_Elf
9 years agosi3144
9 years agocalrosl
9 years agotiredpsych
9 years agoJoeJudgePsy
9 years agonkaebartani
9 years agoAMSaludMental
9 years ago_AGAPIR
9 years agoanaptpinheiro
9 years agoDerekGriffin86
9 years agorezgid
9 years agoScarletang100
9 years agomuzafferkaser
9 years agoProfRobHoward
9 years agokate17929
9 years agoSameiHuda
9 years agoMonyaMyms
9 years agoazenhba
9 years agolyssa_maniai
9 years agobrontemcleod
9 years agoagnesvirtually
9 years agopishnotposh
9 years agopishnotposh
9 years agoMental_Elf
9 years agotalkJenny
9 years agoBZamora321
9 years agomorriseric
9 years agocorkett_ruth
9 years agoIramnN
9 years agoIain_caldwell
9 years ago_Lowri_Jones
9 years agoCharlotteEP28
9 years agoCarla_McEnery
9 years agoLeeTomlinson8
9 years agoSameiHuda
9 years agoSamei Huda
9 years agoPEFtrace
9 years agoSameiHuda
9 years agoKakieVee
9 years agoJolandaBatist
9 years agovalidconsent
9 years agoJoeBarnby
9 years agoAayushiChatur
9 years agoYasTheLaz
9 years agoSt_Dymphna2
9 years agoAspieMum
9 years agojeff_jeffmarsh
9 years agoMental_Elf
9 years agodoctorafran
9 years agoVoeten1
9 years agoAliciaRidout
9 years agoJasTay10r
9 years agoLapsableReality
9 years agoLapsableReality
9 years agochrisdjtaylor
9 years agojenniey1
9 years agoNHFTNHSLibrary
9 years agoUCLPsychiatry
9 years agoLyndaMaguire
9 years agoJeanStafford_
9 years agoSlowMoTherapy
9 years agoMentalhealthMSc
9 years agoSchrebersSister
9 years agojamiebarsky
9 years agoKOlgah
9 years agoKarl_Tooher
9 years agocsmony
9 years agoMental_Elf
9 years agoFewingsBj
9 years agoChris_d_graham
9 years agoFrancesca_Solmi
9 years agoMental_Elf
9 years agofionaturner13
9 years agoAGIP_Therapy
9 years agoAGIP_Therapy
9 years agosportspsycoach
9 years agojmpsychotherapy
9 years agodannysummer08
9 years agoAndy__Bell__
9 years agoAlisonLRDaSH
9 years agoagalappatti
9 years agoSimonMHR
9 years agoian_hamilton_
9 years agovaughanbell
9 years agoIzzy192451
9 years agoMental_Elf
9 years agoWalrathis
9 years agodrrachelbrand
9 years agoCarla_McEnery
9 years agomkennedyswits
9 years agoSciSeekFeed
9 years agoTime4Recovery
9 years agoHersteltalent
9 years ago