
The benefits and risks of antidepressants continue to be hotly debated, both in the scientific literature and in the media.
An adverse effect that has been frequently discussed in the past year has been withdrawal symptoms, experienced when stopping antidepressants.
Recognition of these symptoms in the scientific literature is not new; they have been recognised since the early use of tricyclic antidepressants, though there has been debate around their prevalence, severity, and how quickly they resolve.
A recent review, commissioned by the All Party Parliamentary Group for Prescribed Drug Dependence, has addressed a lot of these questions. James Davies and John Read have examined the literature on prevalence of withdrawal symptoms, and severity. This was heavily featured in the media, with statements made such as Antidepressant withdrawal ‘hits millions’ (BBC) and Now doctors MUST wake-up to the dangers of patients hooked on depression pills (Daily Mail).

Methods
The authors state this is a systematic review, with evidence compiled according to the standard PRISMA guidelines. They used a systematic search of the literature, using Medical Subject Headings to identify relevant papers.
Results
- They identified studies of incidence of withdrawal symptoms, from randomised controlled trials, naturalistic studies and surveys
- Pooling data together, they found an estimated incidence of 56%. In other words, more than half of people who take antidepressants experience withdrawal
- They excluded studies they considered outliers, in terms of reported withdrawal symptoms
- They then used survey data to estimate the degree of severity of withdrawal symptoms
- They excluded randomised controlled trials and naturalistic studies from this analysis, as they felt they were biased, because they were short-term in nature, funded by the pharmaceutical industry, or the authors had significant conflicts of interest.

Conclusions
The reviewers concluded that:
- Over half of people taking antidepressants experience withdrawal symptoms
- The severity of these symptoms is severe in over half of cases.
Strengths
- A strength of the current study is the attempt to synthesise what is a very heterogeneous set of data, from a number of sources
- The questions they address are highly relevant, given the number of people being offered antidepressant medication and have been relatively neglected in high quality studies.
Limitations
However, there are a number of limitations which reduce the utility of this review:
Literature search
The reviewers claim to have conducted a “systematic search” of the literature, looking for relevant studies to include in their review. This consisted of a MeSH search (no freetext searching) of MEDLINE, plus searches of PsychInfo and Google Scholar, as well as some citation searching. Any information scientist worth their salt would suggest other databases that are likely to yield further relevant research (e.g. Embase and the Cochrane Central Register of Controlled Trials). It’s highly likely that this “systematic” review does not include all of the published research in the field, and there’s no evidence that the reviewers did anything to look for unpublished research.
Inclusion criteria
There is no evidence that the systematic review inclusion criteria was registered in advance (pre-registration is designed to prevent changes to methodology once researchers have had a look at the data). From the paper it is not clear if factors such as length of follow-up, length of antidepressant exposure, or drug company funding were defined as reasons for exclusion before undertaking the search and data extraction.
The authors describe exclusion of “outlier” studies which report withdrawal incidence at 11-12% because they assessed “only 9 withdrawal symptoms”, but this outcome measure is not totally at odds with some of the papers they do include. They also exclude a number of studies, summarised by Baldwin and colleagues (Baldwin, 2007), which report withdrawal in the range 6.9% (escitalopram) to 32.7% (paroxetine). Had these studies been included in the analysis, estimates of 11-12% would no longer constitute outliers.
Assessment of study quality
Review articles are notoriously difficult to interpret, and this led to the setting of defined criteria for reviews, which have been called “systematic reviews.” This requires the authors to evaluate study quality, based on attempts to control for issues such as selection bias (samples that are not representative of the population of people we wish to examine), or blinding (whether the participant or the observer knows they are receiving the intervention or not). This is part of the PRISMA checklist, subsumed under the heading, “risk of bias”. This review does not attempt a traditional assessment of bias in the studies they include. These measures enable study quality to be examined, as lower quality studies will invariably produce biased results.
Though the authors make a point of identifying studies funded by drug companies, and where there are potential conflicts of interest related to pharmaceutical companies, they do not assign measures of study quality across studies, and ignore a number of potential biases, such as selection bias.

Conflict of interest
Whilst identifying conflicts of interest related to drug companies, ideological or intellectual conflicts of interest are not discussed. As Ioannidis (2016) and others have stated, meta-analyses have become a tool for academics with vested interests which might go beyond those tangible conflicts of interest traditionally defined by journals.
Outcome measures
In addressing the first question-incidence/prevalence of withdrawal symptoms, they consider the measure, change in withdrawal symptoms (DESS) as a definitive measure of withdrawal. All measures have weaknesses, and in three of the studies they present, they omit mention that symptoms identified with DESS are also present in those continuing to take antidepressants (Rosenbaum et al., 1998; Zajecka et al., 1998; Montgomery et al., 2005). In the Zajecka randomised, double-blind study it is worth noting that the incidence of withdrawal symptoms as measured by the scale is higher in those continuing to take antidepressants (76%), compared to those stopping (67%). It is also worth noting comments made in a paper cited by the authors on the DESS (Hindmarch et al., 2000), “defining a “discontinuation syndrome” as an increase of four or more symptoms…may lead to an overestimation of symptoms.” In fact many of the included studies have an even less stringent cut-off to define “withdrawal”. This is not mentioned at all in the Read and Davies article and therefore gives a particularly misleading account of the Zajecka et al. paper.
Furthermore, withdrawal symptoms themselves are not homogeneous; they vary amongst medications and individuals, and no effort is made to unpick this complexity.

Non-representative surveys to measure incidence/prevalence
Using survey data has strengths and weaknesses. A strength is the large numbers of people that fill out online surveys. However, a major concern is whether they are representative of the population of interest (i.e., all people prescribed antidepressants). A standard methodology for online surveys is to assess the completion rate, i.e., those who were offered the survey, and those who completed it (Fincham, 2008). But this is not possible with the internet methodology used in all of the surveys included in this review. A potential bias from online surveys is that they will be filled out by a specific group of people (this is seen frequently with polling surveys). Anyone conversant with UK politics will have seen this phenomena over the last few years.
This does not mean that the views of people who complete online surveys are not relevant (they are) and they provide important information about the qualitative nature of withdrawal symptoms in some individuals. However, they cannot provide a valid estimate of the frequency of withdrawal symptoms in people who stop taking antidepressants. Many journals will not publish surveys if it is impossible to gauge the response rate or response representativeness (Cooke et al., 2000).
When addressing the issue of severity of withdrawal symptoms, the authors only consider survey data. The reason given, is that a lot of the randomised trials and naturalistic studies are short-term, or at risk of potential bias owing to conflicts of interest. However, if they are using these studies for the quantification of withdrawal effects, and the data is valid for that purpose, it is baffling why it would not be valid for reporting severity; scrutiny of these studies commonly shows lower severity compared to survey reports. It would have been legitimate, for example to report withdrawal severity from included studies, and then stratify for type of study.

Data extraction and presentation of results
There are mistakes in their reporting of a number of studies included in the review:
- In the Montgomery study, the incidence of withdrawal symptoms following escitalopram treatment is presented as 27%, when it is 16%.
- There are 97 people in the Bogetto study, rather than the 95 they report.
- There are 8 patients prescribed paroxetine in the Tint et al., study, rather than 9.
- The Hindmarch and colleagues paper was published in 2000, rather than 2017.
- The total number experiencing withdrawal in the study by Sir and colleagues is 83 rather than 110.
Whilst each of these errors is minor, it does not point to rigorous quality checking by the authors, reviewers or journal editorial staff. Also, where there are errors in reporting the incidence of withdrawal symptoms they are in the direction of symptoms being more frequent; thereby favouring the authors’ view.
Mixing study designs
It is questionable how the authors can justify combining data from randomised controlled trials and naturalistic studies, conducted under study conditions, with survey data. All methodologies have their strengths and weaknesses, though combining data from different methodologies is unconventional, and rarely seen in peer-reviewed literature.
In the presentation of the results of the review, there is no measure of how consistent results were between individual studies. We have tried to address this below.

Combining data from different types of antidepressants
Another potential limitation is the combining of antidepressants with different pharmacokinetic properties, i.e., different ways of being metabolised by the body. For example, fluoxetine has a half-life of 4-6 days after chronic use (active metabolite half-life 4-16 days) compared to paroxetine (approximately 21 hours) and venlafaxine (approximately 5 hours). There is fairly strong evidence to suggest that medications with longer half-lives will be associated with less withdrawal effects, so it is puzzling that the results are presented for all antidepressants combined.
Related to this is the lack of any discussion about the pharmacology of antidepressants and mechanisms for withdrawal, which would have been helpful in explaining the results. Particularly, if a large minority of patients are experiencing symptoms for longer than 3 years (as described in Davies et al 2018) the mechanism for this needs to be understood.
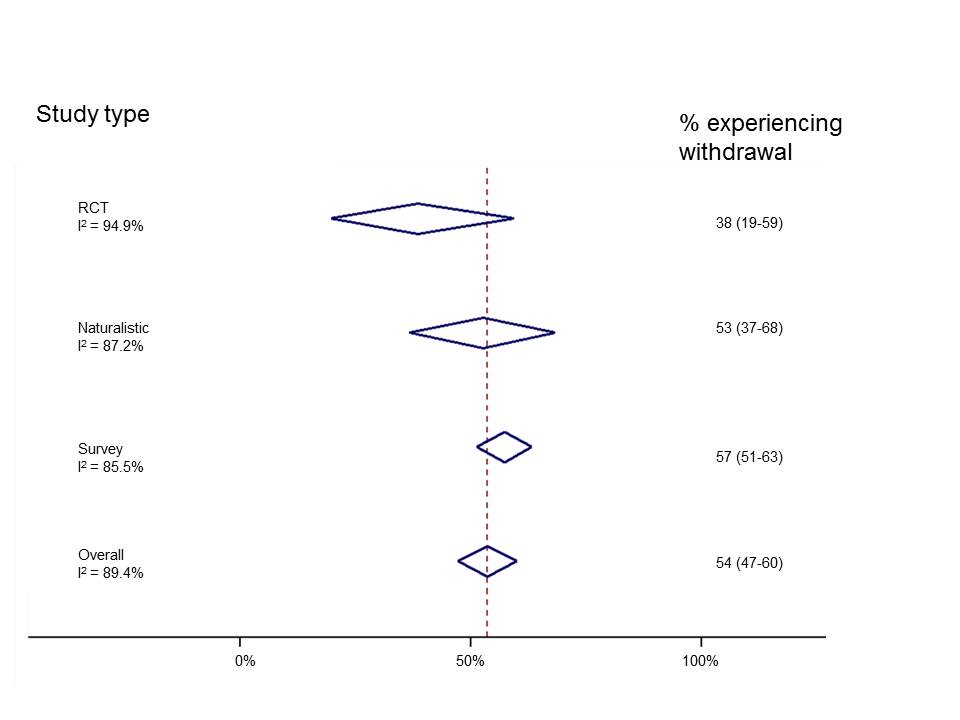
Reanalysis
Given the limitations discussed we urge caution in the interpretation of the incidence/prevalence and severity rates presented. However, we reanalysed only the studies included by Davies and Read in their assessment of incidence (whilst incorporating the corrections we note above) to highlight a number of important points. We organised studies by study type and found that reports of withdrawal events were highest in surveys and lowest in RCTs. Also, we can see (from the measure called I2) that results of individual studies are highly inconstant (I2 can range from 0%-100% and NICE classes I2 of more than 75% “very serious heterogeneity” and would downgrade the meta-analysis for this because there is no precise estimate of withdrawal occurrence). This suggests that combining study designs does not make statistical sense.
We can do something similar, but this time sorting by antidepressant (though combining studies across different study designs).
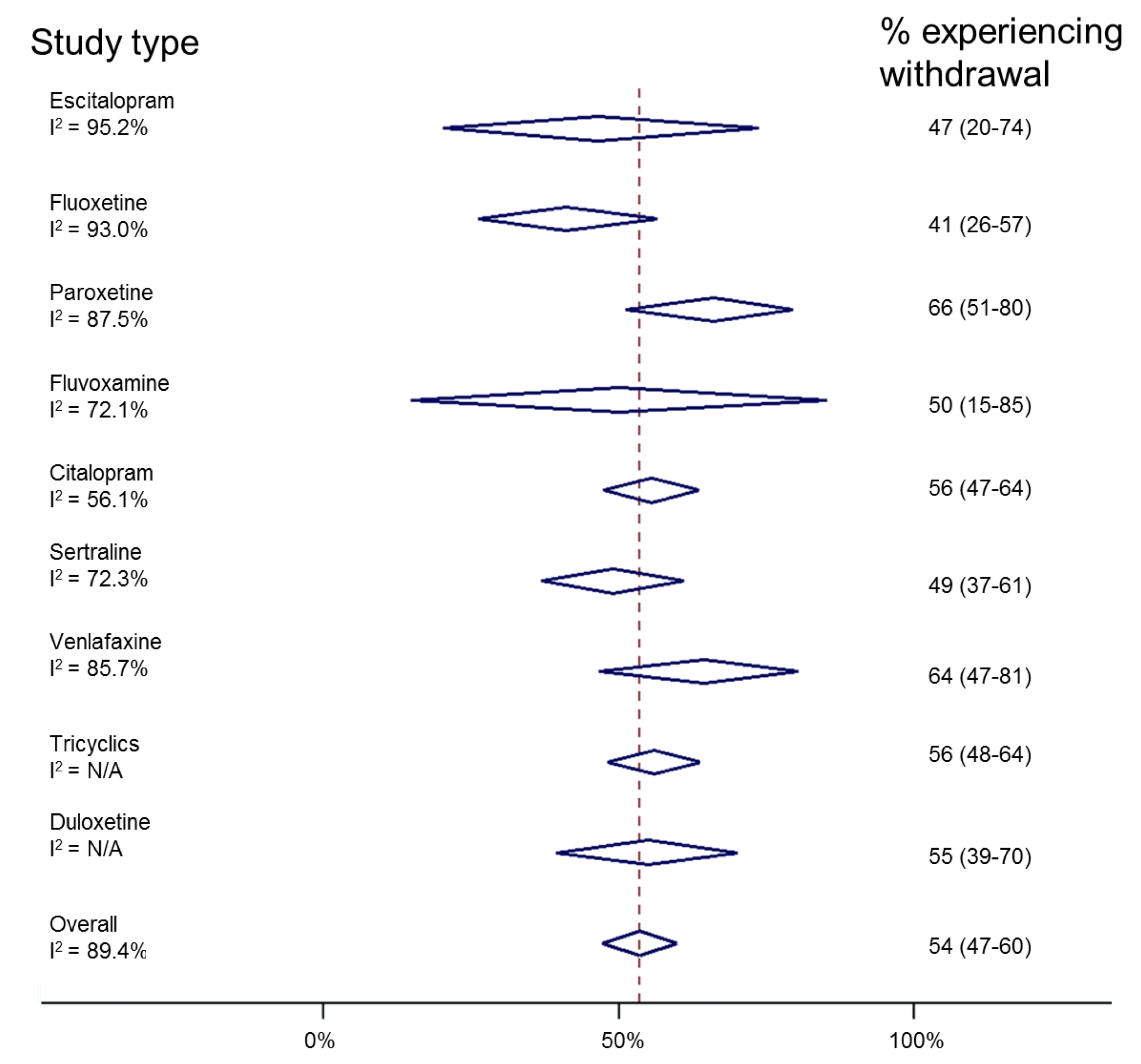
Similarly, this shows huge inconsistencies between individual studies. However, it suggests that paroxetine and venlafaxine are associated with withdrawal most commonly, and fluoxetine least commonly. This reflects experience in clinical practice and is useful information “hidden” in this review. Ideally, one would look at drug effects in different study designs, though there are insufficient numbers of studies to do this reliably.
Implications for practice
The headlines that followed the release of this review were very clear. They stated that half of people taking antidepressants would experience withdrawal symptoms, and that most people reporting withdrawal symptoms class them as severe.
Looking carefully at the review, it does not accurately portray the data.
Whilst withdrawal effects are high for certain drugs (paroxetine, venlafaxine), when stopped abruptly, this happens very rarely in clinical practice and guidelines are in placed to address this. Furthermore, if people do experience withdrawal symptoms, there are treatments available, such as cross-titrating to a drug with a longer half-life, less likely to cause withdrawal, such as fluoxetine, followed by tapered withdrawal.
The issue of time course of withdrawal is not addressed in the review, but will merit careful analysis of the trial and study evidence, as well as that reported in surveys, where the length of follow-up may well be longer.
In conclusion, this is a very topical review, and the authors no doubt have the very best of intentions in communicating their analysis of data. However, the non-systematic way in which the review is written, with errors in data extraction and interpretation make it difficult to accept the findings with any confidence. It reflects negatively on the whole of the field of psychiatry that there is not better, clearer evidence from high quality studies on the incidence, severity and duration of any symptoms related to antidepressant cessation.
Conflicts of interest
Joseph Hayes is funded by the National Institute for Health Research (NIHR) Biomedical Research Centre at University College London Hospital and UCL, and the Wellcome Trust. He has never received drug company funding. He is a Consultant Psychiatrist.
Sameer Jauhar is funded by the National Institute for Health Research (NIHR) Biomedical Research Centre at South London and Maudsley NHS Foundation Trust and King’s College London, and a SIM Fellowship from the Royal College of Physicians, Edinburgh. He has never received drug company funding. He is a Consultant Psychiatrist.
Links
Primary paper
Davies J, Read J. (2018) A systematic review into the incidence, severity and duration of antidepressant withdrawal effects: Are guidelines evidence-based? (PDF) Addictive Behaviors. 2018 Sep 4. https://doi.org/10.1016/j.addbeh.2018.08.027
Other references
Baldwin DS, Montgomery SA, Nil R, Lader M. Discontinuation symptoms in depression and anxiety disorders. International Journal of Neuropsychopharmacology. 2007 Feb 1;10(1):73-84.
Cook C, Heath F, Thompson RL. A meta-analysis of response rates in web-or internet-based surveys. Educational and psychological measurement. 2000 Dec;60(6):821-36.
Mayor S. (2016) Five minutes with… John Ioannidis. BMJ
Davies, J et al. (2018) A survey of Antidepressant Withdrawal Reactions and their Management in Primary Care. Report from the All Party Parliamentary Group for Prescribed Drug Dependence.
Fincham, J. E. (2008) Response Rates and Responsiveness for Surveys, Standards, and the Journal. American Journal of Pharmaceutical Education, 72(2).
Montgomery, S. A. et al. (2005) ‘A 24-week randomized, double-blind, placebo-controlled study of escitalopram for the prevention of generalized social anxiety disorder’, The Journal of Clinical Psychiatry, 66(10), pp. 1270–1278.
Rosenbaum, J. F. et al. (1998) ‘Selective serotonin reuptake inhibitor discontinuation syndrome: a randomized clinical trial’, Biological Psychiatry, 44(2), pp. 77–87.
Zajecka, J. et al. (1998) ‘Safety of Abrupt Discontinuation of Fluoxetine: A Randomized, Placebo-Controlled Study’, Journal of Clinical Psychopharmacology, 18(3), p. 193.
de Vrieze J. (2018) Meta-analyses were supposed to end scientific debates. Often, they only cause more controversy. Science, 18 Sep 2018.
Photo credits
- Photo by rawpixel on Unsplash
- Gerald Leonard CC BY 2.0
- Photo by Steve Johnson on Unsplash
- Photo by David Pisnoy on Unsplash
- Photo by imgix on Unsplash



Withdrawal/discontinuation effects of antidepressants – Inside Health 22/10/19 | Margaret McCartney's Blog
6 years agoAntidepressant withdrawal: slower and lower tapering of SSRIs
7 years agoAltostrata
7 years agojames davies
7 years agoAltostrata
7 years agoAndre Tomlin
7 years agoAndre Tomlin
7 years agoMichael Musgrove
7 years agoanne
7 years agoAndre Tomlin
7 years agoDr. James Davies e Prof. John Read Respondem à Crítica do ” Mental Elf” | Mad In Brasil
7 years agoThomas Steven Roth, MBA, MD
7 years agoPeter J Gordon
7 years agoPost Of The Week – Sunday 21st October 2018 | DHSB/DHSG Psychology Research Digest
7 years agoJohn
7 years agoBracken12345
7 years agoDr Neil MacFarlane MRCPsych
7 years agoConcernedCarer
7 years ago