
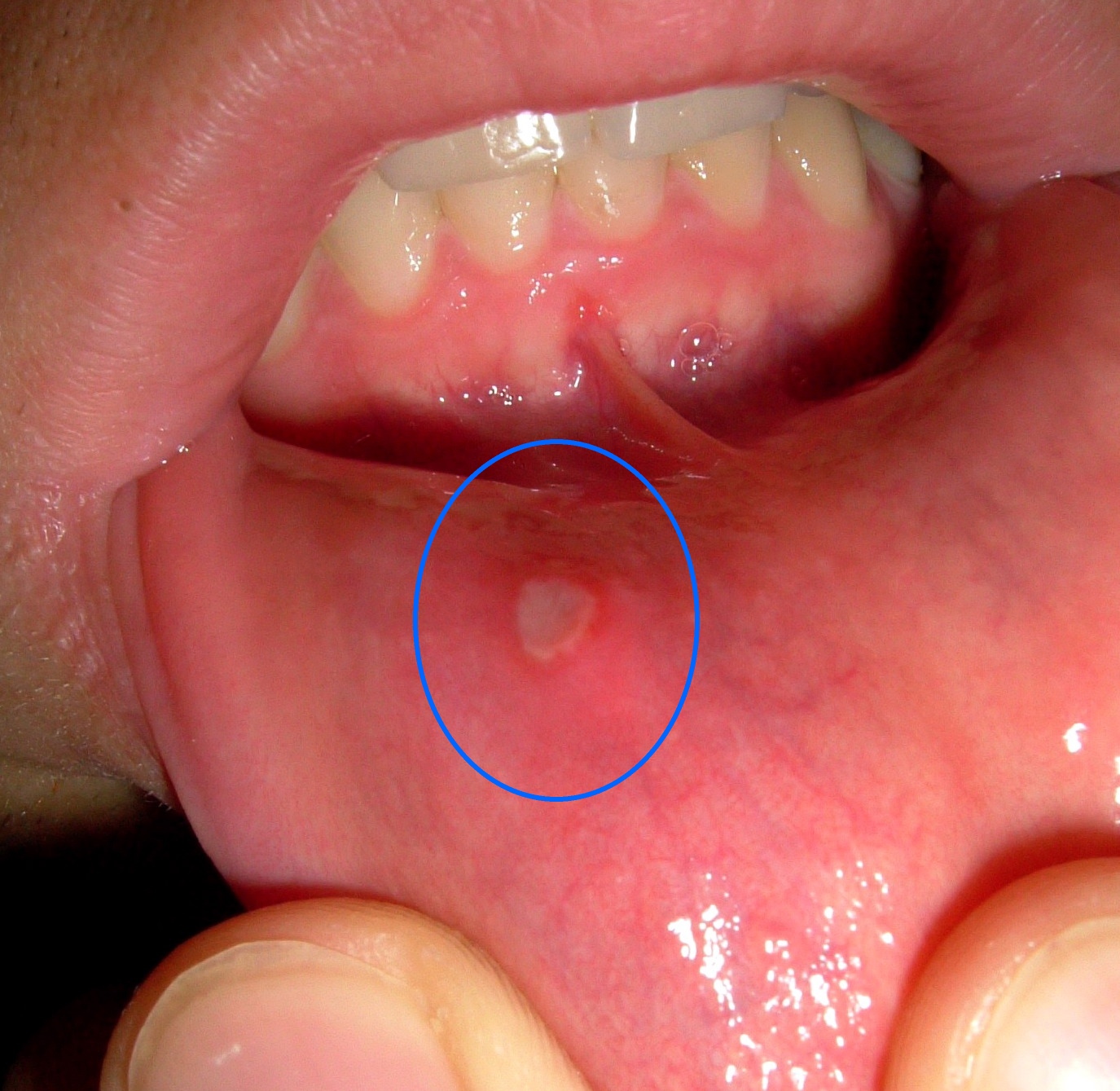
Recurrent aphthous stomatitis (RAS) or recurrent aphthous ulcers are common with the 2012 Cochrane review (Dental Elf – 14th Sep 2012) reporting prevalence estimates ranging from 5-60%. Three forms are recognised minor, major and herpetiform with a peak age of onset of 10-19 years of age although they can persist into adulthood. Their aetiology and pathogenesis is not fully understood and treatments are mainly symptomatic with the main objectives being, relieve of pain, promoting lesion healing and increasing the interval period. Topical medication, laser, cryotherapy and cautery are considered to be effective topical treatments
The aim of this review was to compare the efficacy and safety of topical interventions used for recurrent aphthous stomatitis.
Methods
A review protocol was registered with PROSPERO. Searches were conducted in the Cochrane Central Register of Controlled Trials (CENTRAL), PubMed, Embase and the Web of Science. Randomised controlled trials (RCTs) of local interventions in patients with a confirmed diagnosis of RAS were considered. Main outcomes were clinical efficacy assessed as ulcer size reduction, symptom reduction and time to healing and safety. Two reviewers screened and selected studies and extracted data. Study quality was assessed using the Cochrane domain-based approach. Standard pairwise and network meta-analysis were conducted. Risk difference (RD)with 95% confidence intervals (CI) was used for dichotomous variables and mean difference (MD) with 95%CI for continuous variables
Results
- 72 studies were included including 3 three-arm studies and 2 four-arm studies.
- Most studies involved patients with minor RAS.
- Patients ages ranged from 6.8 to 71 years.
Healing effect (26 RCTs ,1306 patients)
- 14 RCTs (820 patients) were pooled in 7 pairwise comparisons with triamcinolone, laser, silver nitrate, and honey showing a significant preference compared to placebo.
- A network meta-analysis (NMA) of 26 RCTs) showed shorter healing times and better healing effects relative to placebo for honey, insulin liposome gel and laser with no significant differences for other comparison.
- Compared to placebo the interventions were ranked in order as Insulin-liposomal gel, honey, laser, penicillin and aloe.
Size-reducing effect (37 RCTs, 3587 patients)
- Data from 23 RCTs (1807 patients) were pooled in 8 eight pairwise comparisons for size-reducing effect triamcinolone, probiotics, glycyrrhiza and amlexanox were significantly better than placebo.
- Data from a NMA of 37 RCTs suggested that amlexanox, glycyrrhiza and triamcinolone were more effective than placebo with no significant differences for other interventions.
Symptom-reducing effect (46 RCTs, 4020 patients)
- 9 pairwise comparisons (32 RCTs 2940 patients) were pooled for symptom-reducing effect. Triamcinolone, laser, glycyrrhiza, amlexanox and aloe were considered superior to placebo.
- Data from a NMA of 46 RCTs suggested that Amlexanox, laser and triamcinolone have a significant advantage over placebo with no statistically significant differences for other interventions.
Conclusions
The authors concluded: –
most of the local interventions did not show significant differences in the efficacy evaluation and safety evaluation. Based on the currently available evidence, we recommend the use of laser as a short-term intervention to promote healing and reduce pain during the exacerbation phase of RAS and probiotics as a long-term intervention to prolong the inter-episode period and reduce recurrence during the exacerbation and remission phases of RAS. We call for more large-scale RCTs based on trustworthy standards.
Comments
10 years have now elapsed since a Cochrane review looked at systemic treatment for recurrent aphthous stomatitis (Dental Elf – 14th Sep 2012) and since then this blog has looked at a number of other reviews of specific topical and systemic interventions (Dental Elf RAS blogs). This new review had a protocol published on the PROSPERO database and searched a good range of databases for RCTs of topical treatments for RAS. The reviewers identified 72 studies examining some 29 interventions , including placebo, allicin, aloe, amlexanox, benzydamine, berberine gelatin, chitosan chlorhexidine, clobetasol, cryotherapy, curcumin, dexamethasone, diosmectite, doxycycline, glycyrrhiza, honey, insulin-liposomal gel, laser, minocycline, N-acetylcysteine, penicillin, probiotics, prostaglandin E2, quercetin, silver nitrate, sucralfate, triamcinolone, triester glycerol oxide and zinc. Of the 72 studies 23 were assessed as being at high risk of bias and only 4 at low risk with the remainder being at unclear risk. A number of the interventions were only tested in single RCTs and there is variation in the format, dosage and delivery and duration of the interventions in the included studies. In addition, studies on the recurrence of RAS are lacking. So, while this review provides a helpful overview of topical interventions that have been used for RAS the findings should be interpreted cautiously because of limitations in the quality of the evidence.
Links
Primary Paper
Liu H, Tan L, Fu G, Chen L, Tan H. Efficacy of Topical Intervention for Recurrent Aphthous Stomatitis: A Network Meta-Analysis. Medicina (Kaunas). 2022 Jun 7;58(6):771. doi: 10.3390/medicina58060771. PMID: 35744034; PMCID: PMC9227309.
Other references
Dental Elf – 14th Sep 2012
Dental Elf RAS blogs
Picture Credits
https://commons.wikimedia.org/wiki/File:Aphthe_Unterlippe.jpg, CC BY-SA 3.0,



{kind=link}