


Before we start I have to disclose I am a great believer in cognitive behavioural therapy (CBT) delivered using digital technology. I have sat through many clinics seeing patients over and over again who were in what felt like a perpetual holding pattern waiting for psychotherapy and never quite getting it, in spite of my many referral letters. In fact, this got to be so frustrating that I started a company that develops applications to deliver these and other types of non-pharmacological treatments. The need for therapy is such that there is no other way to reach the millions that need it.
Fairburn and Patel (2014) discuss the methods to disseminate psychological treatments globally and come to the conclusion that computerised self-delivered or facilitated treatments are one of the key ways to reach all of those who need it and the only method that really scales.
Internet cognitive behavioural therapy (iCBT) has been shown to be effective (Andersson and Cuijpers, 2009), and it can scale up with minimal resources, but the key question has remained whether iCBT can get participants to complete the treatment.
To answer this question van Ballegooijen and colleagues undertook a meta-analysis of studies investigating face to face and internet based CBT for depression looking in particular at treatment completion and length of treatment for those that discontinue it (Ballegooijen et al. 2014).

Methods
The authors primarily examined www.evidencebasedpsychotherapies.org an existing database that aims to list all trials for psychological treatments for depression. According to the authors the database was current as of January 2013. They identified 14,164 abstracts from 4 major databases. They also looked into PhD theses, but it is not clear how they did this. They stated that they did not seek out other unpublished studies due to time constrains.
For the meta-analysis they included studies on CBT among depressed adults (18+ years). These adults either had gone through a diagnostic interview or scored above cut-off on a validated symptom scale. They included studies where one arm was either CBT or iCBT but the iCBT had to have a coaching component by telephone, email or some means of communication, completely self-administered therapy was not included. The authors also excluded studies where depression was co-morbid with other conditions and studies published before 2000 as that is when research on iCBT started. They also excluded studies which combined therapy with medication and studies on group CBT. They only looked at community studies where participants had been recruited through advertising rather than through clinical services.
Coding
The main outcome was average number of sessions/modules completed by participants divided by the total number of sessions. Where authors defined ‘completion’ as going through a number of sessions lower than the specified maximum number that was the number used in the above calculation. The authors state that this could overestimate completers in the CBT condition. Two raters independently carried out data extraction.
Quality assessment
As efficacy outcomes were not analysed, the authors only carried out quality assessment on how completion of sessions was recorded and how missing data were dealt with. Two independent raters did the quality assessment and they resolved disagreements through discussion.
Meta-analysis
The authors assessed heterogeneity using the I2 statistic and a random effects model. Each outcome measure was pooled within the face to face and iCBT subgroups and the final analysis was done using a mixed effects model with fixed effects for the analysis within the subgroups and random effects for the between subgroups analysis.

Results
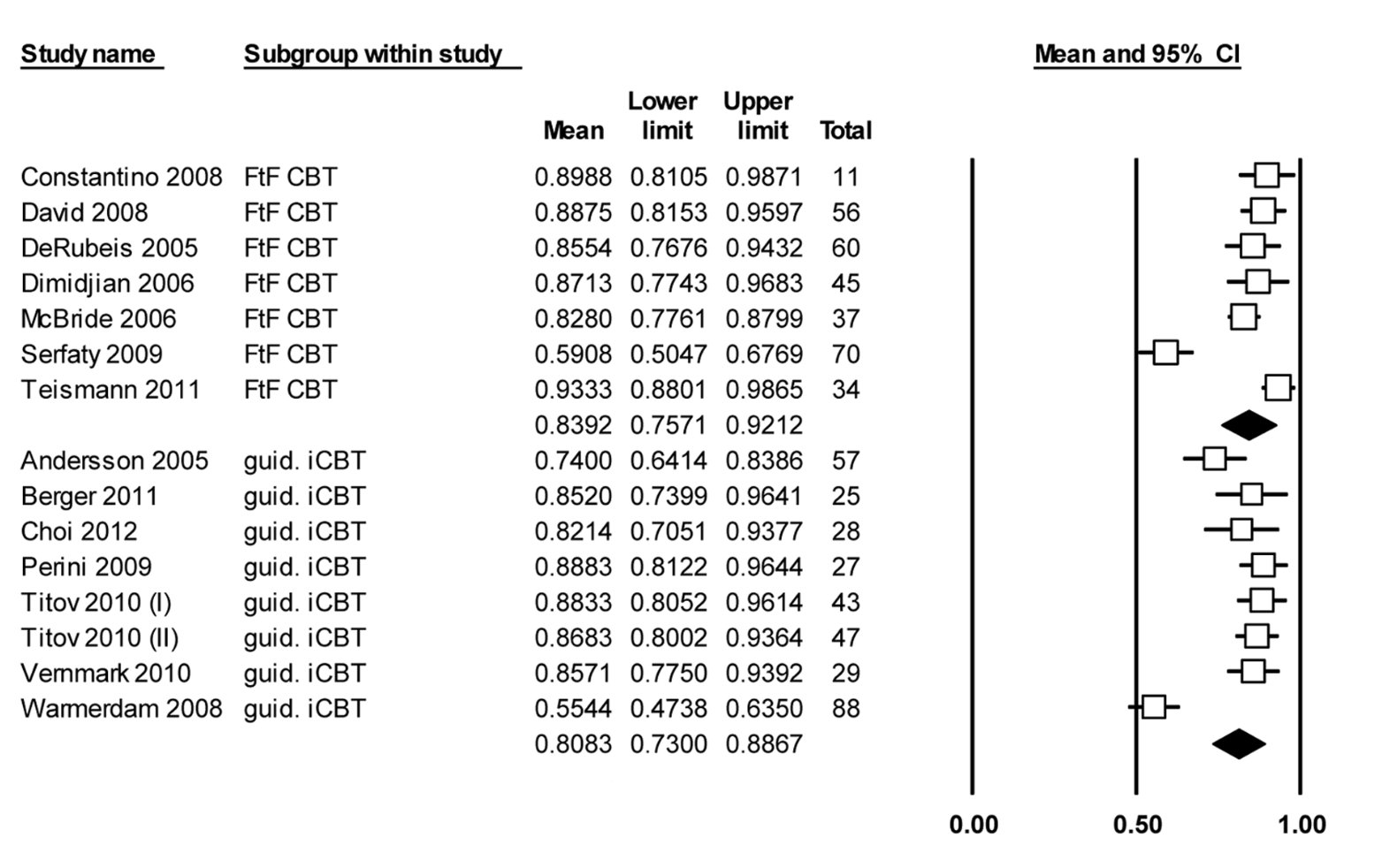
After running through the exclusion criteria the authors identified 24 papers describing 26 treatment conditions and extracted 14 treatment conditions for face to face CBT and 12 for iCBT. There were no papers comparing iCBT with CBT directly.
- CBT ranged from 12 to 28 sessions and iCBT interventions consisted of 5 to 9 sessions
- CBT participants completed on average 83.9% of their treatment, which did not differ significantly from participants in guided iCBT who completed 80.8%
- The percentage of completers was significantly higher in CBT (84.7%) compared with iCBT (65.1%, P = .001)
- The percentage of completers of 80% or more of the intervention was significantly higher in CBT (85.2%) compared with iCBT (67.5%, P = .003)
- Non-completers of face-to-face CBT completed on average 24.5% of their treatment, while non-completers of guided iCBT completed on average 42.1% of their treatment.
Discussion
The study focused on adherence to guided iCBT as compared to face to face CBT. The authors chose guided iCBT as opposed to unguided on the presumption that guided CBT yields better results and better treatment adherence (Andersson and Cuijpers 2010; Richards and Richardson 2012).
However, when directly comparing guided and unguided iCBT in the same trial, the intervention rates of adherence did not differ greatly (Berger et al. 2011). The study was not designed to look at adherence so it may have been underpowered, but it may be that adherence is more related to study population or intervention design.
In most trials of iCBT (guided and non-guided) reasons for discontinuation are usually not reported and there is no analysis on what factors may contribute to greater adherence within the intervention itself or intrinsic to the participants. There is also one study that suggested participants in an unguided programme dropped out because they had recovered.
Limitations
- The studies included were very heterogeneous (various designs, lengths of treatment and definitions for ‘completion’) and there were no studies directly comparing guided iCBT with face to face CBT.
- The final number of studies was small and while there was a difference in the main outcome measured it did not reach significance. This might have been because the meta-analysis was underpowered.
- Having said this, the authors’ choices when coding completion in face to face CBT, may have resulted in artificially higher completion rates in that group.

Conclusions
After reading this study I believe guided iCBT offers lower adherence than face to face CBT judging by the percentage of 100% and 80% completers. Interestingly, the average number of completed sessions was similar in both groups, which seems to be explained by the percentage completed by those who did not finish the treatment, which was higher in the guided iCBT group.
Investigation into what can be done to re-engage after discontinuation in guided iCBT (and non-guided) might be a fruitful line of research.
There was no economic analysis accompanying the meta-analysis but it is safe to assume that the cost of delivering guided iCBT is lower than that of CBT.
We need to focus on what specific adherence mechanisms result in better outcomes and we need to produce more studies comparing guided and unguided iCBT and also direct comparisons between CBT and iCBT.
I believe this method still holds much promise. The efficacy of iCBT is fairly well established by now with the caveat that people going through it need to complete it to benefit. We need to focus on what specific strategies can maximise adherence, particularly to non-guided iCBT as it is likely to be the most scalable method of reaching the maximum number of people at the lowest cost.

Links
van Ballegooijen W, Cuijpers P, van Straten A, Karyotaki E, Andersson G, et al. (2014) Adherence to Internet-Based and Face-to-Face Cognitive Behavioural Therapy for Depression: A Meta-Analysis. PLoS ONE 9(7): e100674. doi:10.1371/journal.pone.0100674
Andersson G, Cuijpers P (2009) Internet-based and other computerized psychological treatments for adult depression: a meta-analysis. Cognitive Behavioural Therapy 38: 196–205 [PubMed abstract]
Berger T, Hammerli K, Gubser N, Andersson G, Caspar F (2011) Internet based treatment of depression: a randomized controlled trial comparing guided with unguided self-help. Cognitive Behaviour Therapy 40: 251–266 [PubMed abstract]
Clarke G, Kelleher C, Hornbrook M, Debar L, Dickerson J, et al. (2010). Randomized effectiveness trial of an Internet, pure self-help, cognitive behavioral intervention for depressive symptoms in young adults. Cognitive Behavioural Therapy 38: 222–234 [PubMed abstract]
Fairburn C G, Patel V (2014). The Global Dissemination of Psychological Treatments: A Road Map for Research and Practice. American Journal of Psychiatry, 171(5), pp. 495–498 [PubMed record]
Richards D, Richardson T (2012) Computer-based psychological treatments for depression: a systematic review and meta-analysis. Clin Psychol Rev 32: 329–342. [PubMed abstract]





Computerised CBT (cCBT) for depression and anxiety in youth
10 years agoBest in Mental Health (weeks of 12/8/2014 - 12/21/2014) - SocialWork.Career
11 years agoBest in Mental Health (weeks of 12/8/2014 - 12/21/2014) - Social Work Career.Tips
11 years agoMy Shrink Is Trying To Poison Me
11 years agoJenny_Edwards
11 years agoJenny_Edwards
11 years agofelly500
11 years agowendypots
11 years agowendypots
11 years agoBABCP
11 years agoheleenriper
11 years agoFageMD
11 years agoJoão Leal
11 years agoNicola Davies
11 years agoPhysiowizz
11 years agoOTBeth131
11 years agocaputpurgijs
11 years agoRecoveryRay
11 years agoOHcounseling
11 years agoPeteQYork
11 years agoMental_Elf
11 years agoCCreswell99
11 years agoJoanneYounge
11 years agoJoanneYounge
11 years agoJoanneYounge
11 years agosandycann2
11 years agosoniajohnson
11 years agoBwoodHighland
11 years agoAriesStudyUCL
11 years agosuzypuss
11 years agoMental_Elf
11 years agohelencoulshed
11 years agoMDPWellness
11 years agoaghoury79
11 years agoatimeforbalance
11 years agoTaylorAlanJ
11 years agosuzypuss
11 years agojenwild1
11 years agoangela_sheard
11 years agoMental_Elf
11 years agoBarbieBFlove
11 years agoTravisHillLPC
11 years agoKayFSheldon
11 years agoserenderen
11 years agoLucyDPlymUni
11 years agoMNazir9
11 years agoCaffeineAndHate
11 years agoHealthwatchCov
11 years agojanemccourt1
11 years agohubgodalming
11 years agoCommLinksTrain
11 years agoChrissyOzolins
11 years agoMental_Elf
11 years ago121Therapy
11 years agoHHLibService
11 years agoHelen_OTUK
11 years agomhresources
11 years agoBigWhiteWall1
11 years agomidstaffsmindb1
11 years agoMental_Elf
11 years agoCYPSNEP
11 years agoMental_Elf
11 years agoBABCP
11 years agoAndy Conway
11 years agoMental_Elf
11 years agoLisa Eden
11 years agoThe Mental Elf
11 years agocolinlever
11 years agoAmanda Collins-Eade
11 years agoKirsten Corden
11 years agoIain_caldwell
11 years agocaputpurgijs
11 years agoKeelingJoanne
11 years agoCrossCrissy
11 years ago