


For people who are suffering from a severe depression, antidepressants are a very effective treatment, but how they work is still not fully understood. The basic biochemistry of how one dose of the drug affects one part of the nervous system is known, e.g. increasing serotonin levels at the synapse by preventing it from being recycled into the neurons (SSRIs), but this is a far too simplistic account of what will be happening in the brain in order for these drugs to be effective. Neuroimaging offers another way to try and understand the effects of these drugs on how the brain functions at a wider level.
People who are depressed have difficulties with a number of different neuropsychological tests looking at negative and positive emotions. During a depressive episode, on average, people:
- Process negative stimuli differently:
- Pay more attention to negative emotions
- Remember negative stimuli better
- Classify neutral/ambiguous faces as negative
- Remember more negative events from the past
- Process positive stimuli differently:
- Classify positive faces as neutral
- Experience reduced pleasure from previously rewarding activities
- Struggle to regulate emotions as well, especially getting control of negative emotions
When people recover from depression these biases in their emotional processing improve a lot. Previous studies have suggested that changes in the emotion processing areas in the brain underlie this improvement (no matter what treatment is offered).

To work out how antidepressants might be affecting the neural circuits that underlie emotional processing a researcher from Baltimore performed a meta-analysis of studies where people did an emotional processing task during an MRI scan. We have discussed meta-analyses of functional MRI studies before and there are real technical challenges combining lots of different studies using different scanners and analysis methods. Over the last couple of years most people have converged on using one technique (www.brainmap.org/ale) and this new study uses it.
Methods
A literature search found studies looking at two types of antidepressants: SSRIs (e.g. fluoxetine) and SNRIs (e.g. venlafaxine). Only studies that directly looked at the difference between taking antidepressants and not were included, i.e. studies where:
- The same person took an antidepressant and then a placebo (or vice versa) sequentially,
- A group taking an antidepressant were compared to a group taking placebo
- Comparing people before and after taking an antidepressant
Both healthy people and people experiencing depression were included to see if there are differences in how antidepressants affect their brains.
Sixty studies were included with 1,569 participants. The tasks that people performed in the scanner were broadly similar: emotional stimuli were presented to them in various different ways.
Brain imaging studies do a lot of statistical comparisons. The problem with this is that if you stick to p=0.05 for accepting/rejecting each test then you would expect 1 in 20 tiny areas of the brain to be ‘significant’ even if none of them are actually true (false positives). This study took account of this by setting acceptable error rate by using a method called the false discovery rate. This reduces the significance level of each individual test so that overall the chance of a positive finding for the whole brain not being really true (false positive rate) remains at the standard 1 in 20, or p<0.05.
Results
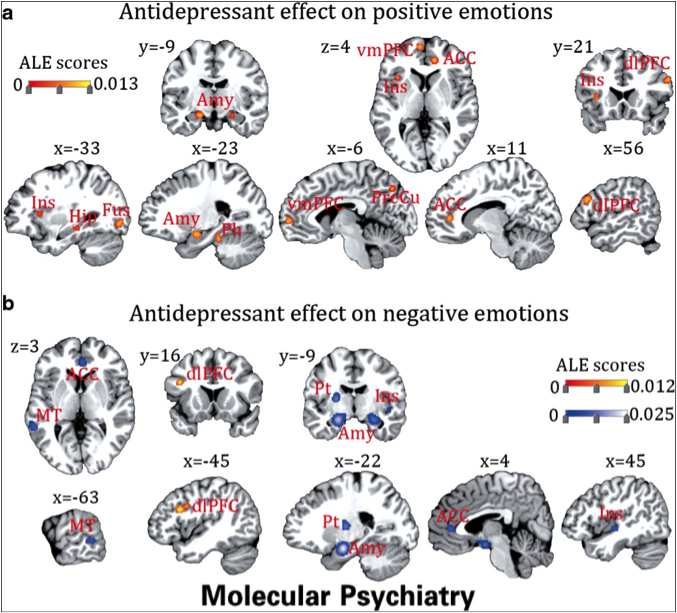
In people who are suffering from depression, taking antidepressants regularly:
- Decreased the response of the brain to negative emotional stimuli
- Increased the response of the brain to positive emotional stimuli
- Increased the activation of an area of the prefrontal cortex linked to emotional regulation
Figure one shows the details of where these changes took place, but in summary, areas of the brain long know to respond to emotional stimuli were affected.
Figure 1: Red indicates increased activity, blue decreased
In healthy volunteers, taking antidepressants regularly:
- Decreased responses to negative emotional stimuli
- BUT a decreased response to positive emotional stimuli was found
- AND there was no effect in the prefrontal cortex
- The study showed that similar areas of the brain were affected by the drugs
One dose (usually very high) of antidepressant had a different effect:
- There were both increases and decreases to both positive and negative emotional stimuli, even within the same network within the brain
Conclusions
The author concluded:
Antidepressants act to normalize the abnormal neural responses in depressed patients through reduction of mood-congruent biases by increasing activity to positive emotions and decreasing activity to negative emotions in the amygdala, insula and anteriour cingulated, and increasing regulatory responses in dlPFC [part of the prefrontal lobe].
He also argued that the study suggests that antidepressants work primarily by altering the emotional processing biases, rather than boosting emotional regulation, and that this suggests that antidepressants and CBT could be complementary, as CBT focuses much more on emotional regulation.
Summary
- People who are depressed have well described biases in how they process emotional stimuli in the environment
- Antidepressants help to correct these biases, and this study suggests that this is the main mechanism of action
- Giving people who are depressed the space to not be focusing on negative emotions or events all the time is a powerful first step to help people make changes in their lives to sustain their recovery
- To have a sustained positive effect, antidepressants need to be taken regularly, as one-off doses have a much more mixed effect on emotional processing. This may underlie the increased agitation and anxiety that some people, but not all, experience when starting an antidepressant
- Healthy people taking antidepressants regularly may experience a reduction in the emotional reactivity of the brain

Link
Ma Y. Neuropsychological mechanism underlying antidepressant effect: a systematic meta-analysis. Mol Psychiatry. 2014 Mar 25. doi: 10.1038/mp.2014.24. [PubMed abstract]




Best in Mental Health (weeks 6/9 - 6/22/2014) - SocialWork.Career
11 years agoSJohnstonPsy
12 years agoDeborahEllisWC1
12 years agoDr Roland Bessis
12 years agowaddellae
12 years agoStellaWYChan
12 years agoStellaWYChan
12 years agosteveflatt
12 years agopharmagossip
12 years agoSameiHuda
12 years agoKirsten Corden
12 years agoCandace Alexandra Price
12 years agoIain_caldwell
12 years agocrayfish27
12 years agoGill_Livingston
12 years ago121Therapy
12 years ago121Therapy
12 years agoMoiraBrimacombe
12 years agotombssimon
12 years agodarrensolutions
12 years agoOPDI
12 years agoMandyware
12 years agoprofelainefox
12 years agohullodave
12 years agoMental_Elf
12 years agoBarrell7Paul
12 years agoConor Saunders
12 years agoSJS_31
12 years agoJoão Leal
12 years agoalbertmorrison
12 years agoictinpr
12 years agogothemind
12 years agoninnles
12 years agoNeuronet64
12 years agoOrlamhicl
12 years agoMindsWellUK
12 years agostephentimothy
12 years agoCharlieWallerIn
12 years agoRuaidhri_
12 years agoFrankenTan
12 years agoandrot
12 years agotitto4all
12 years agolypftlib
12 years agocognitivecouch
12 years agoBPSOfficial
12 years agoMental_Elf
12 years agowilytwit
12 years agoHHLibService
12 years agoBwoodHighland
12 years agoDaniElOman
12 years agoKeith_Laws
12 years agoSaffMitten
12 years agoCaroline Tomes
12 years agodoctorfreddie
12 years agoMegEliz_
12 years agoRichard Semmens
12 years agoYannnSud
12 years agoMental_Elf
12 years agocialdella01
12 years agoLisa Eden
12 years agoThe Mental Elf
12 years agopsynthesisblog
12 years agoIHAWKES1
12 years agomrsjotaylor
12 years agoWiz_Waz
12 years ago121Therapy
12 years ago