

Diabetes is an increasingly common health condition and individuals with a learning disability are believed to make up a significant number of those adults with diabetes in the UK (Morin, 2012).
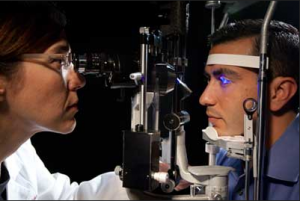
Diabetic Retinopathy is a common complication of diabetes. High blood sugar levels can damage the retina, which is a light sensitive tissue at the back of the eye. This damage can be permanent if not caught early enough. Those at risk should have annual checks and good control of both blood sugar levels, cholesterol and blood pressure to help control the risk of permanent damage to their retinas.
The health inequalities experienced by people with learning disabilities (LD) have been well documented (Emerson et all 2010), especially accessing screening programmes for preventative purposes. Data from GP (General Practice) systems in the UK indicates higher rates of diabetes amongst the learning disabled population, yet lower rates of appropriate screening (Glover, Emerson & Eccles 2012).
The issues that cause low uptake of diabetic eye screening include practical barriers such as support to attend screening, lack of understanding around the importance of the screening process and fear associated with the screening process, concerns regarding capacity to consent and availability of accessible information and resources for screening (Norah Fry research centre, 2013).
In order to facilitate better screening uptake, Turner & Emerson (2013) developed a resource paper outlining reasonable adjustments that should be made to diabetes services for people with leaning disabilities. These include examples of local procedures and make reference to specific accessible resources for his client group.
This paper was followed by a further document which outlines additional adjustments to facilitate the successful screening (Pilling, 2014). These adjustments include highlighting a persons disability at the time of referral, promoting access to screening services, providing accessible information and allowing individuals with a learning disability to have additional time within for the screening process to take place.
Method
The authors’ initial goal was to to find out if people with learning disabilities and with diabetes are getting access to eye screening tests they need to detect potentially dangerous changes in their eye function. The authors undertook an audit in order to find out the numbers of individuals with a learning disability and diabetes have had the appropriate eye screening tests as set out in the NICE (National Institute for Clinical Excellence) guidelines for diabetic patients (2004,2008).
These guidelines currently state that diabetic patients should undergo eye screening at the time of diagnosis and then annually. This is to safeguard against the development of ‘sight threatening’ retinopathy. The screening is photographic, although other screening methods are available for those who are unable to undergo photographic screening.
The authors used a list of adults known to the learning disability health facilitation team in Bradford, Yorkshire and then matched this list of names against the list of adults known to be eligible for diabetic retinopathy screening (sourced from General Practice groups). The resulting list was then used to ascertain the outcomes of screening using OptoMize, the diabetic eye screening programme electronic database (DESP). The following questions were asked:
- Does the diabetic eye screening service in Bradford meet the standards set out by NICE?
- Are reasonable adjustments made to facilitate equality of access for adults with a learning disability?
71 adults with a learning disability and diabetes were identified using the methodology outlined by the authors. The following criteria were set by the authors in order to effectively measure the quality of service and equality of access:
- The patients’ LD was recorded in the ‘cognitive status’ fuels of demographic information.
- Adults with LD who are eligible for screening are offered photographic screening.
- Adults with LD who are eligible for screening have a recorded screening outcome (photographic or other screening method).
- Adults with LD who are unable to undertake photographic screening are offered alternative screening methods.
Results
- 59 per cent had a documented learning disability (41 patients).
- 91 per cent had been offered diabetic retinal screening (64 patients) and of these 74 per cent were under the care of Diabetic Eye Screening Programme (DESP).
- 14 per cent were under the care of the hospital eye department (10 patients).
- A total of 3 per cent were not known to DESP (2 patients).
- Surprisingly for 6 per cent (4 patients) it was unclear who was responsible for diabetic screening.
- 35 per cent of patients did not have a recorded screening outcome (24 people).
When looking at those patients known to the DESP, 26 percent had never completed a diabetic eye disease examination (18 patients). Reasons included failing to attend appointments (16 per cent, 11 patients), being labelled as unsuitable by their GP (6 per cent, 4 patients), attempts to obtain photographs were not successful in 3 per cent (2 patients) and failure to be offered an appointment accounted for 1 per cent (1 patient). Analysis of those patients known to the hospital service indicated that only 3 out of 14 patients who were not able to have photographic screening were offered an alternative method of screening.
In terms of the outcome of diabetic screening for adults with a learning disability recorded in the database since 2010, the following findings were reported:
- 25 per cent (17 patients) have had retinopathy present on at least one screening visit.
- 12 per cent (8 patients) have been referred to the hospital eye clinic for monitoring of sight threatening disease.
- 2 patients subsequently underwent laser surgery to treat the condition.
Conclusions
The authors state that the current audit identified 91% patients had been offered eye screening for diabetic retinopathy and were known to the DESP. However, only 65% of these had a recorded outcome. Therefore, they conclude that the national standard for diabetic eye screening is not being met for adults with a learning disability.

Comments
It is interesting that the authors make a reference to the fact that some GP’s labelled individuals with LD as being ‘unsuitable’ for screening. It seems that despite the advances being made in respect to the autonomy of this client group, there are professionals who see it as acceptable to make decisions on their behalf. The current audit along with the Turner & Emerson (2013) paper outlining reasonable adjustments to diabetes services for people with LD, was used to create a list of recommended practices to improve uptake of diabetic screening in this client group (via focus group and subsequent review by members of Vision 2020 learning disability subcommittee). Since this set of practices was developed at the time the article was written – this audit has lead to the development of new guidance for screening in this client group (Ophthalmic Services Guidance, September 2015) which is an applaudable achievement.
Summary
There are noted barriers to patients with a learning disability and diabetes getting appropriate eye screening in the UK. These include cognitive elements such as understanding the importance of undergoing screening and practical support to attend screening and follow up. There is also the wider issue of the reading rates of diabetes within the population as a whole and within the learning disability community. Therefore, the issue of screening will continue to be important and require attention by health professionals and those supporting people with a learning disability.
Screening requirements should form part of service users Health Action Plans (HAP). Additional work has been identified around helping service users to understand why the screening is required and the practicalities of attending a screening assessment. Examples include developing accessible information and adjustments to the screening process to allow greater levels of participation on the day. Those supporting individuals with a learning disability and diabetes need to be aware of the signs and symptoms of retinopathy, however. The emphasis should remain on early screening once diabetes is diagnosed, over relying on screening once problems are already observed and therefore long term damage may have already occurred.
Links
Primary link
Pilling, R. F (2014). Screening for diabetic retinopathy in adults with learning disability: current uptake and adjustments to facilitate equality of access. British Journal of Learning Disabilities, 43, p 62-65 [Abstract]
The SeeAbility leaflets
Other references
Emerson, E., Baines, S. (2010). Health inequalities and people with learning disabilities in the UK: Durham, Improving Health & Lives, Learning Disabilities Observatory.
Morin, D., Merineau-Cote, J., Oulette-Kuntz, H., Tasse, M,J., & Kerr, M. (2012). A comparison of the prevalence of chronic disease among people with band without intellectual disability. American journal of intellectual developmental disabilities., 117: 455-463. [Abstract]
Glover, G., & Emerson, E., & Eccles, R. (2012). Using local data to monitor the health needs of people with learning disabilities, Durham, Improving Health & Lives: Learning Disabilities Public Health Observatory.
Opthalmic Services Guidance (September 2015). Eye care for adults with learning disabilities. Royal a College of Opthamologists.
Pilling, R.F (2014) Diabetic eye screening in people with learning disabilities: Improving access. Journal of Diabetes Nursing, 18: 199-202.
Turner, S. & Emerson, E. (2013). Making reasonable adjustments to diabetes for people with learning disabilities. Learning disabilities Public Health Observatory.. Department of Health.
Turner, S., Giraud-Saunders, A., Marriott, A. (2013). Improving the uptake of screening services by people with learning disabilities across the south west peninsula: a strategy and toolkit. Norah Fry research centre/National Development Team for Inclusion.




BibSonomy :: url :: Diabetic retinopathy tests accessible to adults with learning disabilities?
10 years agokentautistic
10 years agoISDRstudy
10 years agoZena Olney
10 years agoJIDR_Wiley
10 years agocarterjenny16
10 years agoGwenMoulster
10 years agoLearningDisElf
10 years agoJohnTurnbull20
10 years agoStacey Marie Hurst
10 years agoRobertBalogh1
10 years agoHampshire Healthcare Library Service
10 years agoLearningDisElf
10 years agoRachelRachelj21
10 years agoIOWNHSLibrary
10 years agort_sen
10 years agoHorshamPsychol
10 years agoHorshamPsychol
10 years agoLearningDisElf
10 years agoThe Learning Disabilities Elf
10 years agoKaty Welsh
10 years agoPH_Rochdale
10 years agoDiabetes_Elf
10 years agoBusyOT
10 years ago