
Do you remember 2007? That’s the year Northern Rock collapsed triggering the banking crisis, Amy Winehouse went global with Back to Black, and the final book in the Harry Potter series hit the shelves.
It was also the last time the National Institute for Health and Clinical Excellence (NICE, 2007) published guidance on psychosocial interventions for substance misuse.
A recent review by the NICE project team concluded that:
After considering all the new evidence and views of topic experts, we decided that no update is necessary for the guideline.
– NICE, 2016
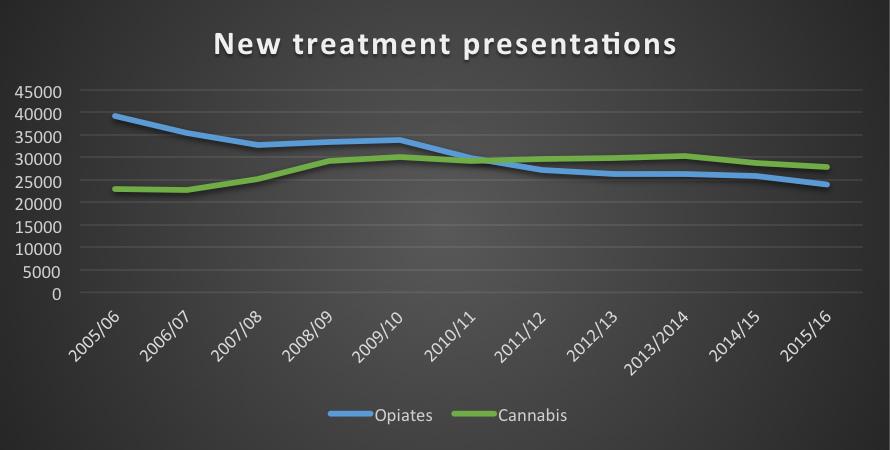
So is guidance published a decade ago fit for purpose in 2016? First it’s important to consider what’s happened with drug use and which drugs people have developed problems with. Back in 2007, opiates such as heroin accounted for the majority of new treatment presentations, but since then cannabis has become the main drug that people present with, as shown in the graph below.
Opiate centric
Although the guidance has some generic information about assessment, self-help, brief interventions and involving families, it is telling that most of the examples given are in relation to injecting. This is important, but gives the impression that the guidance is aimed at ‘high risk’ injecting drug use. The majority of people who develop problems as a result of drug use in 2016 are not injecting their drugs. Cannabis remains the most widely used illicit drug and presentations to treatment services where cannabis is the primary problem have risen significantly in the last decade (Monaghan et al, 2016).
A recent Cochrane review for cannabis dependence found evidence to support a combination of motivational enhancement therapy (MET), cognitive behavioural therapy (CBT) and incentives (Gates et al 2016). But as fellow Elf Mark Monaghan pointed out in a recent blog, these reviews including the one by NICE limit their search to papers published in English (Monaghan, 2016). Given the range of treatment programmes across Europe, it is likely that we are missing valuable intelligence if evaluations of these treatments are published in a language other than English.

Missing themes
Just like mass marketing, generic guidance misses some key groups and topics. Pregnant women who have drug problems are not catered for, but as two lives are involved deserve attention. Unfortunately all females have been ignored in research on substance use as acknowledged by a recent editorial in the Journal of Addiction (Del Boca, 2016).
Since 2007, legal highs or novel psychoactive substances (NPS) have emerged as a group of drugs that cause a range of problems, which workers in a range of settings will encounter. Project Neptune is one example of innovation in the field which offers evidence based guidance on NPS for drugs workers
Misuse of prescription drugs is not mentioned in the guidance, despite recent evidence that across Europe the United Kingdom has some of the highest levels of misuse of these drugs (Novak et al, 2016).
Although the last decade has seen a dramatic reduction in tobacco smoking in the general population this has not been mirrored for people who have problems with drugs, the majority of whom smoke. This is a complex issue for example many treatment staff who may not consider smoking a priority if you are injecting heroin. But research shows this group can be encouraged to quit (McClure et al, 2014).
There is scope for NICE to acknowledge these groups and substances in their updates, which might help draw attention to gaps in research and knowledge.

Digital interventions
The last decade has seen significant innovations in technology. The Mental Elf being a good example of the way information about health and evidence is now communicated. In parallel, online or electronic methods of delivering health care have developed. Breaking Free Online is one example of a drug treatment innovation, which has accumulating evidence of reaching groups that don’t usually access traditional services (Elison et al, 2015).
Limitations
Alcohol is not included in the 2007 psychosocial interventions for substance misuse guidance, although NICE has issued a range of alcohol related guidance. Moreover, people don’t present with neat single drug use problems; they often use multiple substances including alcohol. It might be challenging in terms of drawing up guidance, but if guidance is to be meaningful and used in practice it needs to reflect the problems real people present with.
An additional factor is the relationship between mental health and substance use. Up to 70% of people in drug treatment settings have mental health problems (Turning Point, 2016). Although new guidance is due to be published by NICE imminently on dual diagnosis, topic or issue specific guidance risks looking artificial and distant from the reality of the complex problems that people present to services with. Depending on the individual presentation, a clinician could need to refer to three or more sets of NICE guidance, none of which take account of each other. There must be a better way to support workers and the people they meet.

Summary
When reviewing their guidance, the teams at NICE invite individuals and organisations to submit comments and evidence. The consultation for this review attracted only two stakeholder contributions, but one notable stakeholder did disagree with the NICE decision not to update the guidance: Public Health England.
The overall lack of engagement with NICE on its consultation could be a reflection on the state of the treatment sector. Most drug treatment providers and the specialist staff working in them are subject to frequent retendering exercises. The sector has faced savage cuts in the last decade which have resulted in a rapid turnover of providers and staff. An environment that doesn’t lend itself to engaging with NICE on treatment guidance when survival is the priority.

Links
Primary paper
National Institute for Health and Clinical Excellence (2016) Surveillance report 2016 – Drug misuse: psychosocial interventions (2007) NICE guidelines CG51, 2016.
Other references
Del Boca, F.K., 2016. Addressing sex and gender inequities in scientific research and publishing (PDF). Addiction.
Elison, S., Davies, G. and Ward, J., 2015. Effectiveness of Computer-Assisted Therapy for Substance Dependence Using Breaking Free Online: Subgroup Analyses of a Heterogeneous Sample of Service Users. JMIR mental health, 2(2).
, , , , . Psychosocial interventions for cannabis use disorder. Cochrane Database of Systematic Reviews 2016, Issue 5. Art. No.: CD005336. DOI: 10.1002/14651858.CD005336.pub4.
McClure, E.A., Acquavita, S.P., Dunn, K.E., Stoller, K.B. and Stitzer, M.L., 2014. Characterizing smoking, cessation services, and quit interest across outpatient substance abuse treatment modalities. Journal of substance abuse treatment, 46(2), pp.194-201. [Abstract]
Monaghan,M. (2016) CBT and motivational interviewing: best bet for cannabis cessation. The Mental Elf, 7 Jun 2016.
Monaghan, M., Hamilton, I., Lloyd, C. and Paton, K., 2016. Cannabis matters? Treatment responses to increasing cannabis presentations in addiction services in England. Drugs: Education, Prevention and Policy, 23(1), pp.54-61. [Abstract]
National Institute for Health and Clinical Excellence (2007) Drug misuse in over 16s: psychosocial interventions. https://www.nice.org.uk/guidance/cg51
Novak, S.P., Håkansson, A., Martinez-Raga, J., Reimer, J., Krotki, K. and Varughese, S., (2016). Nonmedical use of prescription drugs in the European Union. BMC psychiatry, 16(1), p.274.
Turning Point (2016) Dual Dilemma (PDF).




The Service Delivery PIG | Dave's Bankside Babble
9 years agoDublinHempCo
9 years agoCommLinksTrain
9 years agoBOPjo_anne
9 years agoandyinhaler
9 years agoRecoveryDoctor
9 years agopamwallace28
9 years agojon_vanniekerk
9 years agoManamaCraven
9 years agoonehandedpotter
9 years agosoniajohnson
9 years agoVanessaLGarrity
9 years agoSaotia_Seay
9 years agoM_Evonda
9 years ago971DXB
9 years agoAPlushsis
9 years agoRigby42881911
9 years agoasuzann98
9 years agoNikkkolassss
9 years agoJacquieWhite7
9 years agoTheRealKairosHD
9 years agoyoboy212
9 years agoBryan135254121
9 years agolaytonbryann
9 years agoBer46603087Ber
9 years agosourcecodeman
9 years agonailahh_j
9 years agofield_matt
9 years agoKMcAdam_SA_MH
9 years agoSian_NP
9 years agomartinsmith02
9 years agoJones23Emma
9 years agotraceyrogers37
9 years agoMHARG_york
9 years ago121Therapy
9 years agoMental_Elf
9 years agoSalPsyAddiction
9 years agosmonnat
9 years agoian_hamilton_
9 years agoMental_Elf
9 years agorecoveringjust1
9 years agoAlcoholHarmCop
9 years agoin2recovery
9 years agomalcolmclayton
9 years agoian_hamilton_
9 years agoMental_Elf
9 years agoDrG_NHS
9 years agoMental_Elf
9 years agoian_hamilton_
9 years agoIan Hamilton
9 years agoChristina Armstrong-Graham
9 years agoThe Mental Elf
9 years agoNICEcomms
9 years agoESRCnewdrugs
9 years agoMental_Elf
9 years agoMental_Elf
9 years agoalteredworlds
9 years agoNHFTNHSLibrary
9 years agoLuke Ricketts
9 years agoJEPettett
9 years agoNICEcomms
9 years agoCJrpeake
9 years agoSectioned_
9 years agoNICEcomms
9 years agoian_hamilton_
9 years agoSectioned_
9 years agoian_hamilton_
9 years agoSectioned_
9 years agoian_hamilton_
9 years agoSectioned_
9 years agoian_hamilton_
9 years agoSectioned_
9 years agoIs NHS guidance on substance misuse fit for purpose? | Public Health News
9 years agoian_hamilton_
9 years agoDRUG_LAW_REFORM
9 years agoSectioned_
9 years agoSectioned_
9 years agoACCymru
9 years agoMHARG_york
9 years agoNEPNHS
9 years agoMental_Elf
9 years agoian_hamilton_
9 years agoGlobalDrugSurvy
9 years agodickonb
9 years agoLucy May Nicholson
9 years agoVoices4ChoicesT
9 years agoVoices4ChoicesT
9 years agojopackaj
9 years agoZoegatland
9 years agoPHI_IMS
9 years agoViralKMH
9 years agoian_hamilton_
9 years agoNICEcomms
9 years agoMHARG_york
9 years agoian_hamilton_
9 years agoHealthSciYork
9 years agojamesmorris24
9 years agopash22
9 years agoian_hamilton_
9 years agoGlyn_Davies1
9 years agonigeldawsoncpc
9 years agoJohnFoster12
9 years agoJohnFoster12
9 years ago121Therapy
9 years agodocjohnnie
9 years agoian_hamilton_
9 years agoian_hamilton_
9 years agoDrugWiseUK
9 years agoian_hamilton_
9 years agoDrugWiseUK
9 years agoian_hamilton_
9 years agoMental_Elf
9 years agoian_hamilton_
9 years agoSMMGP
9 years agoian_hamilton_
9 years agoAGIP_Therapy
9 years agoJohnBaker_Leeds
9 years agoCNWLlibraries
9 years agoGearoid1987
9 years agoRoger Batterbury
9 years agoMental_Elf
9 years agonhslowsecure
9 years agopeteqconsult
9 years agompmon
9 years agopeterleohurst
9 years agoian_hamilton_
9 years agojoannekane1
9 years agoian_hamilton_
9 years agoMHARG_york
9 years agosarahiweld
9 years agoSciSeekFeed
9 years ago