
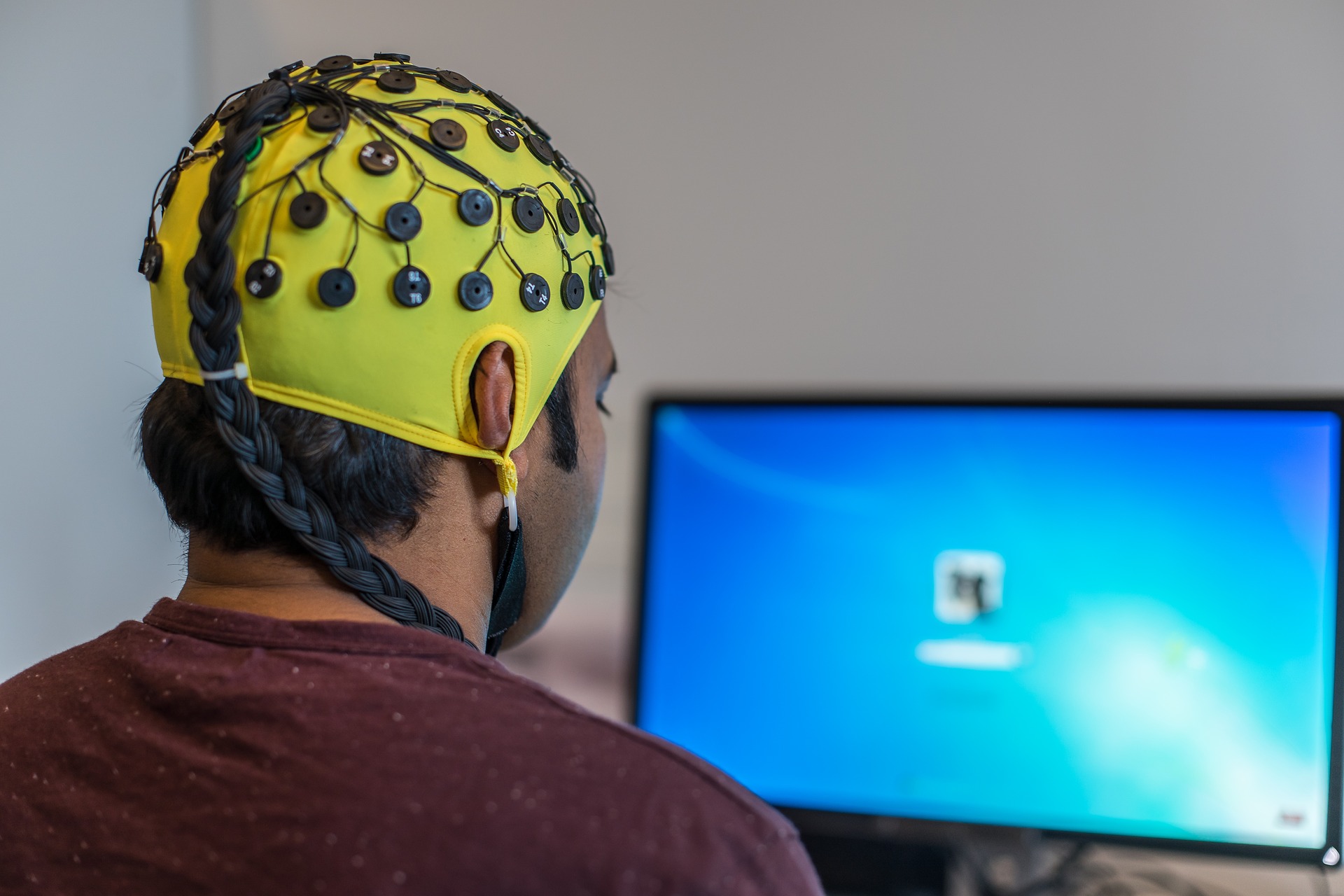
Attention Deficit Hyperactivity Disorder (ADHD) is a neurodevelopmental disorder characterised by persistent inattention, impulsivity, and hyperactivity. Neurofeedback is an intervention designed to alleviate altered patterns of brain activity that are apparent in ADHD. Electroencephalography (EEG) is used to record neurophysiological activity on the scalp, which is then presented on a visual display. The individual’s aim is to increase the signal in a certain brain region or frequency band that is associated with ADHD, thereby normalising brain activity.
We blogged last year about a meta-analysis of neurofeedback for ADHD in children, which concluded that neurofeedback cannot currently be recommended as a treatment for children with ADHD.
Summarised below are the methods and findings of a randomised controlled trial (RCT) of neurofeedback for adults with ADHD, conducted by Schönenberg and colleagues (2017) in Tübingen, Germany.
Methods
Adults with ADHD between the ages of 18 and 60 years were recruited for the study. Participants were enrolled if they met the DSM-IV-TR criteria for ADHD and had no or stable use of medication for 2 months, with no intention to change. ADHD diagnoses were confirmed with two self-report scales and a diagnostic interview. Exclusion criteria were severe mental health comorbidities, epilepsy, traumatic brain injury, and substance abuse.
118 eligible participants were randomly allocated to three treatment groups:
- Neurofeedback (n=38)
- Sham neurofeedback (n=39)
- Meta-cognitive therapy (n=41).
Neurofeedback was delivered in 30 bi-weekly sessions. EEG was recorded at the vertex and participants were instructed to enhance beta activity, typically reduced in ADHD, and suppress theta activity, typically increased in ADHD. Positive feedback was given 80% of the time in the form of moving bubbles on a screen when activity was above/below an adaptive threshold. The sham neurofeedback group underwent the exact same procedure, however the feedback they received for the first 15 sessions was pre-recorded from an individual in the actual neurofeedback group. For the final 15 sessions, the sham group received actual neurofeedback.
Meta-cognitive therapy was delivered in 12 weekly group sessions and aimed to provide skills and strategies in time-management, organisation, and planning. CBT techniques were incorporated into the meta-cognitive therapy sessions to address depression and anxiety. Participants were told that they would either receive neurofeedback or meta-cognitive therapy, and they were not aware of the sham neurofeedback condition. The neurofeedback trainer was also blinded, and therefore not aware if the participant was receiving real or sham neurofeedback.
Assessments were conducted at pre-treatment, mid-treatment (after 8 weeks), post-treatment (after 16 weeks), and 6 months later by clinicians who were blind to group assignment. Measures included self-reported adult ADHD symptoms, depression, and state anxiety; neuropsychological assessments of sustained attention (CPT), interference control (Stroop), and cognitive flexibility (TAP and INKA); and theta-beta power ratios recorded with EEG. Treatment effects were analysed by comparing the whole time course across groups.
Results
113 participants (64 men, 49 women) completed the full course of treatment: neurofeedback (n=37), sham neurofeedback (n=38), and meta-cognitive therapy (n=38). The groups were roughly similar in age, education, IQ, ADHD symptoms, ADHD medication, and comorbidities. The findings showed that:
- All groups reported significantly decreased ADHD symptoms over time
- All groups reported significantly improved inattention, hyperactivity, and impulsivity
- All groups reported significantly less anxiety and depression symptoms
- Performance on neuropsychological assessments of interference control and cognitive flexibility, but not sustained attention, significantly improved over time
- There were no significant changes in theta-beta power ratio over time
- The groups did not differ in how much they changed over time on any of the measures.
Conclusions
Large and equivalent treatment effects were found for all groups, suggesting that neurofeedback is not superior to meta-cognitive therapy. No evidence was found to support the purported mechanisms of neurofeedback.
Strengths and limitations
Blinding, randomisation, and good sample size were the main strengths of this study. Blinding eliminated the possibility of experimenter bias and both neurofeedback groups believed they were receiving actual treatment, equating for expectations. The researchers used stratified randomisation to ensure that the groups were similar in gender, age, and ADHD severity. A thorough screening process also ensured that the sample was relatively homogeneous by confirming ADHD diagnosis, keeping medication stable, and excluding major comorbidities.
A significant limitation was the decision to treat the sham neurofeedback group with actual neurofeedback for the second half of the treatment period. In effect, both groups received actual neurofeedback that only differed in dose, i.e. 15 versus 30 neurofeedback sessions. Dose effects are more difficult to find and this may explain why there was no difference between these groups at post-treatment and 6-month follow-up. Only the measures taken at mid-treatment can inform us about the relative efficacy of real versus sham neurofeedback, although these are short-term and only after the half-course of treatment. Nevertheless, a specific comparison of mid-treatment outcomes may have found neurofeedback to be superior to sham, if it was tested.
The neurofeedback protocol was similar to previous studies, but it is interesting to note that EEG was recorded at the vertex, rather than a region implicated in ADHD, and that positive feedback was given 80% of the time. It is debateable how much can be learnt about controlling the theta-beta power ratio with such a high feedback ratio, and this may explain the absence of improvement. In addition, the sham group would have received positive feedback that was consistent with their theta-beta power ratio 64% of the time, and therefore their learning was not greatly different to the experimental group. In fact, the increase in consistency of feedback when they received actual neurofeedback may have been noticeable and attributable to the treatment’s efficacy. This could explain why the sham group improved the least at mid-treatment and the greatest at post-treatment and 6-months.
A final limitation was the absence of a passive control group. This data would have been useful to estimate the natural course of adult ADHD, regression to the mean, and test-retest effects, so that the specific effects of treatment could be determined.
Summary
The findings of this study cast doubt on the purported mechanisms of neurofeedback and undermine its validity as a treatment. Despite this, neurofeedback was associated with large treatment effects; but these were not superior to meta-cognitive therapy, which is shorter and more cost-effective. Careful examination of the long-term efficacy of neurofeedback compared to sham would be warranted, as it may have potential as an alternative or complementary treatment.

Links
Primary paper
Schönenberg M, Wiedemann E, Schneidt A, Scheeff J, Logemann A, Keune PM, Hautzinger M. (2017) Neurofeedback, sham neurofeedback, and cognitive-behavioural group therapy in adults with attention-deficit hyperactivity disorder: a triple-blind, randomised, controlled trial. The Lancet Psychiatry (9), 673-684. Published: 09 August 2017 DOI: http://dx.doi.org/10.1016/S2215-0366(17)30291-2
Photo credits
- [Public domain], via Wikimedia Commons




{kind=link}
Morven Fyfe
6 years ago