

People in England and Wales with an active mental health problem, who are considered to show signs of risk to themselves or others, located in a public space, are sometimes apprehended by police and brought to a safe place under the auspices of the Mental Health Act for assessment and treatment. The power to do this is defined in section 136 of the Mental Health Act. Detention by police, conveyance to a designated 136 “suite”, lengthy assessments by nursing, medical and social care staff, and ensuing use of inpatient care, is extremely costly and labour-intensive, and tends to be reserved for the most acutely unwell people.
In 2013, the then Care Minister Norman Lamb announced several regional pilots of “street triage”, with a view to improving the experiences of people with mental health needs who end up interacting with police and caring professions (Department of Health, 2013). Street triage is a strategy to reduce 136 admissions, which involves having a mental health professional, typically a nurse travel with police officers and assess people, who might otherwise be candidates for 136 arrest, and instigate treatment.
March 2016 saw the publication of an NHS commissioned evaluation of the nine pilot schemes in England, which included quantitative and qualitative data analysis (Reveruzzi & Pilling, 2016). This evaluation concluded: “All but two of the nine Street Triage schemes resulted in a reduction in the use of s136 detentions, when compared with an equivalent timeframe from the previous year.”
The study that is the focus of this blog, published in BMJ Open in November 2016, quantitatively describes a street triage service in the North East of England, and the effect that this service had on the use of section 136 in that region (Keown et al, 2016).
Methods
The investigators present data on a street triage service that was established in the Northumberland, Tyne and Wear in September 2014. They examined street triage engagements in the first year after starting the service, and report uses of the 136 power for the same period, and use the same information for the year prior to September 2014 for comparison. Because the implementation of street triage was staged, starting first in the South of Tyne area, researchers make comparisons between 136 use in areas where street triage was in use with those areas where it had not yet started.
Data on admissions and uses of other Mental Health Act powers is also presented. Rates of street triage engagement are reported, based on estimates of population at risk from the Office for National Statistics.

Results
- The investigators found that use of Section 136 in the study area went down throughout the whole trust
- During first year, the rate of street triage was 138.7 per 100,000 people in the population
- The rate of S136 detentions fell:
- from 59.8 per 100,000 population prior to the introduction of street triage,
- to 26.4 per 100,000 in its first year,
- a reduction of 55.9%
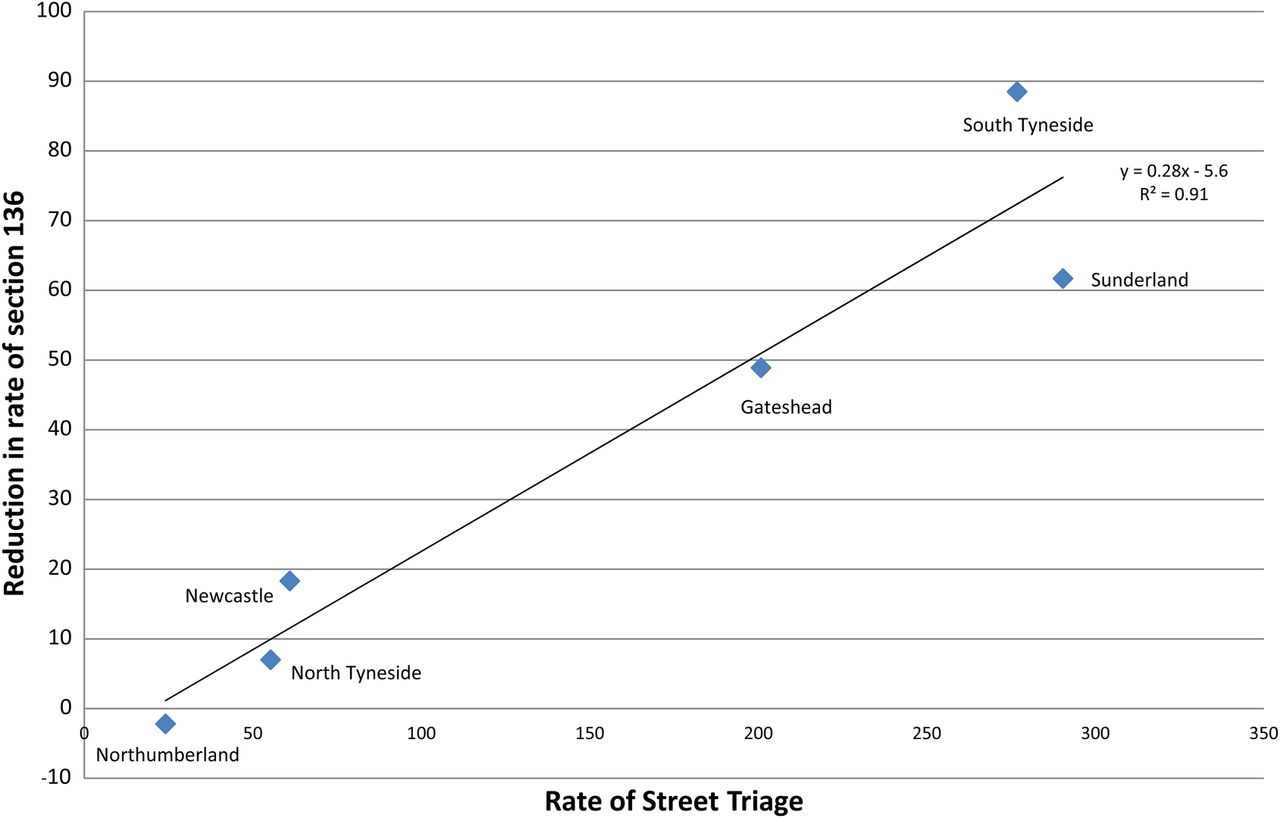
- Areas with more street triage engagements also experienced greater reductions in 136 rate
- Closer examination of street triage areas where a year of data was available, suggested that the reduction of 136 use was spread throughout the year
- Against the background of rising accident and emergency (A&E) attendances throughout the trust in this period, 136 assessments in A&E also fell
- Outcomes of 136 assessments did not change over the study period.
Reproduced from the paper, the authors show this scatter plot of reduction of 136 rate against the rate of street triage, based on six areas in Tyne and Wear:
Conclusion
The authors conclude:
Street triage leads to a reduction in 136 detentions.
Strengths and limitations
Indeed, the analysis is based on a large, densely populated geographic area, with a high background rate of 136 use. Statistical hypothesis testing suggested large differences in 136 rate in the before versus the after period. Given that 136 did not fall in areas where street triage was not happening, an effect of street triage on 136 seems plausible, under the assumption that nothing else important changed in those particular areas over the study period, that might have affected the occurrence of 136 detentions.
However, this assumption doesn’t seem to be covered in much detail in the paper. What information there is in the paper, indicating that one 136 suite closed during the study period, might be expected to reduce the detention rate on its own, although possibly not enough to account for the extent of change observed in this analysis.
Although the geographical area is large, the rate across six units is analysed, limiting statistical power. It is possible that had other units from neighbouring regions been sampled in the study, the association might have been different. There isn’t a great deal of information on measurement in this study; for example were street triage engagements more likely to be recorded correctly in areas with lots of police activity?
There are also important issues with generalisability here. There was not much description of the street triage intervention, so we do not know how this may be different to street triage in other areas, including how it was experienced by patients and the public. Finally, this study did not randomise units to the intervention, and there were only 6 units analysed, so we cannot be sure that it was street triage that was having the effect, and not other background factors. This means that the use of the quantity “number needed to triage”, which assumes a causal effect, is premature. However unlikely it might be, confounding factors that resulted in a reduction in 136 activity cannot be discounted as a cause for these results. Furthermore, it is very unclear how the changing demographic, local policy, and mental heath landscape might have influenced the results.

Implications
The main implications for this study are for research. Reducing section 136 use would appear to have been treated as an adverse outcome in this study, but is that necessarily true? Research on 136 needs to broaden out to adopt a variety of different approaches, with an emphasis on routine data and the experiences of patients. This must take the form of better descriptions of who is detained using this Section and for what reasons, in order to identify what reasonable clinical outcomes we should be measuring.
In clinical practice, we see many patients who, without the use of 136 powers, would not have seen a clinician until much further into an episode of illness. In a resource-poor NHS, how realistic it is to comprehensively roll out mental health staff to accompany police officers remains to be seen.

Links
Primary paper
Keown P, French J, Gibson G, et al. (2016) Too much detention? Street Triage and detentions under Section 136 Mental Health Act in the North-East of England: a descriptive study of the effects of a Street Triage intervention. BMJ Open 2016;6:e011837. doi:10.1136/bmjopen-2016-011837
Other references
Mental Health Act 1983: Section 136.
Department of Health (2013) Extending the street triage scheme: new patrols with nurses and the police.
Heslin M, Callaghan L, Barrett B, et al. (2016) Costs of the police service and mental healthcare pathways experienced by individuals with enduring mental health needs. The British Journal of Psychiatry 2016: bjp. bp. 114.159129.
Reveruzzi B, Pilling S. (2016) Street Triage Report on the evaluation of nine pilot schemes in England (PDF). Department of Clinical, Health and Educational Psychology, University College London




Joan Stock
9 years agoE
9 years agoAdult Mental Health Update
9 years agoPaul
9 years agoMichael Brown
9 years ago