
Bottom line
The recommendations for fallow time in dental practice following an AGP appears almost random in its application across half of international guidelines. Its basic idea appears to be centred on a single precautionary principle based on simulation studies that are only weakly supported by evidence. Policy makers will need to take a more balanced approach when assessing the benefits and harms fallow time creates.
Introduction
With the publication of, ‘Aerosol Generating Procedures and their Mitigation in International Dental Guidance Documents – A Rapid Review’ by the COVID-19 Dental Services Evidence Review (CoDER) Working Group (Clarkson et al., 2020) it was interesting to note their finding regarding fallow time for non Covid-19 patients:
- 48% of the guidelines recommend having a fallow period.
- The amount of time recommended varied (2-180 mins) between guidelines and also within guidelines, depending on environmental mitigation.
- None of the fallow period recommendations referenced any scientific evidence.
The fallow period is the ‘time necessary for clearance of infectious aerosols after a procedure before decontamination of the surgery can begin’ (FGDP, 2020), and this has caused considerable discussion/stress amongst the dentist returning to practice after lockdown in the UK (BAPD, 2020, Heffernan, 2020).
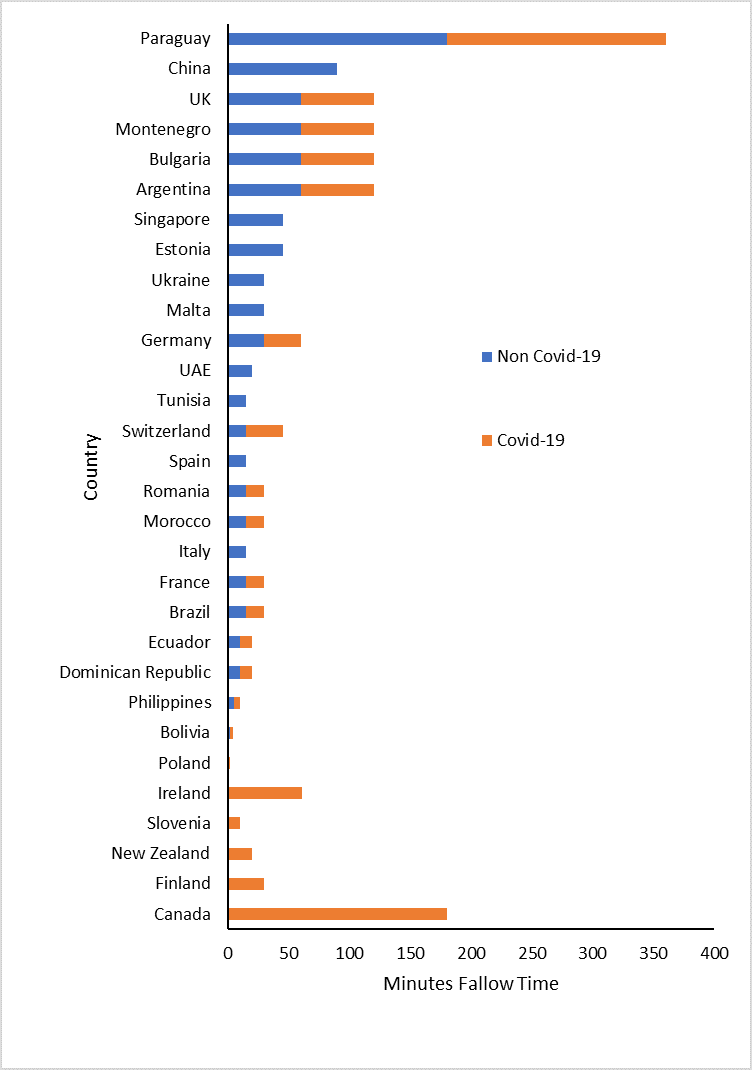
The fallow times following an AGP for both Covid-19 negative patients and Covid-19 positive patients are presented in Figure 1 and Table 2 using the data from the CoDER rapid review:
Figure 1. Stacked bar chart representing fallow times for both Covid negative and positive patients
Since the fallow times are not normally distributed the median value was utilised and the 95% confidence limit approximated according to Hill (Hill, 1987).
Table 1. Median fallow time
| Aerosol generating procedure | Median Fallow time (mins) |
| Non Covid-19 patient | 15 (95% CI: 15 to 30) |
| Covid-19 positive patient | 20 (95% CI: 10 to 60) |
Much of the theory around the need for fallow time is based on the aerosol transmission of the Coronavirus SARS-CoV-2 and the need to allow the aerosol to settle or be physically removed from the room via ventilation or filtration. Initially the WHO supported the idea that spread was predominantly caused by large droplets and contact (WHO, 2020a) but under increased lobbying from the scientific community to include airborne transmission as a significant factor (Morawska and Milton, 2020) the WHO amended their position (WHO, 2020b) on the 9th July.
The evidence for airborne transmission of Coronavirus SARS-CoV-2 is uncertain and mostly based on mathematical modelling (Buonanno et al., 2020) but where there has been limited observational data Hota and co-workers concluded that the virus was not well transmitted by the airborne route compared to measles, SARS-1 or Tuberculosis (Hota et al., 2020).
The reason there is no strong scientific evidence for fallow time and airborne transmission is possibly because it is based on two conceptual arguments:
The Precautionary Principle (PP)
The precautionary principle (PP) states that if an action or policy has a suspected risk of causing severe harm to the public domain (affecting general health or the environment globally), the action should not be taken in the absence of scientific near-certainty about its safety. Under these conditions, the burden of proof about absence of harm falls on those proposing an action, not those opposing it (Taleb et al., 2020). The confusion at the moment is that the PP has been reversed and the action is evidence-based ‘normal/enhanced PPE and cross infection policy’ rather than the imposition of untested application of ‘fallow time’ in general practice.
The Independent Action Hypothesis (IAH)
The IAH states that each virion has an equal, non-zero probability of causing a fatal infection especially where airborne spread via small droplets (5μm) is the proposed method of transmission (Stadnytskyi et al., 2020). The reality of the IAH is that evidence supporting this theory is oversimplified and indirect, based mainly on small sample studies of moth larvae, and tobacco mosaic virus (Zwart et al., 2009, Cornforth et al., 2015).
Discussion
The main problem for anyone challenging the PP and IAH is having to prove a ‘near certainty of safety’ when there are many confounding factors in play, and the application of a ‘non-zero’ probability of a single inhaled virus causing death results in an ill-defined probability of risk (Taleb et al., 2020). Unfortunately, once the PP was been invoked designing challenge studies to create the scientific proof that the action is safe can be unethical in humans or experimentally impossible due to the effect of low viral prevalence in the community on statistical power.
One solution may be to rapidly assess the retrospective infection rates associated with the provision of dental care in those countries with extended fallow times and compare then to countries of similar demographics that do not have fallow time (Table 1). Policy makers may need to revise their current interpretation of the precautionary principle and IAH based on the fact that in a pandemic situation there may be multiple interacting factors that can cause significantly more second and third order harm to the public domain than the virus itself.
Table 2. Countries with/without(bold) fallow time. ND – no data
| Country | Non Covid-19 | Covid-19 | Country | Non Covid-19 | Covid-19 | |
| Ireland | 0 | 60 | Burkina Faso | ND | ND | |
| Poland | 0 | 0 | Canada | ND | 180 | |
| Bolivia | 2 | 2 | Chile | ND | ND | |
| Philippines | 5 | 5 | Columbia | ND | ND | |
| Dominican Republic | 10 | 10 | Costa Rica | ND | ND | |
| Ecuador | 10 | 10 | Croatia | ND | ND | |
| Brazil | 15 | 15 | Denmark | ND | ND | |
| France | 15 | 15 | Finland | ND | 30 | |
| Italy | 15 | ND | Greece | ND | ND | |
| Morocco | 15 | 15 | Guatemala | ND | ND | |
| Romania | 15 | 15 | Honduras | ND | ND | |
| Spain | 15 | ND | India | ND | ND | |
| Switzerland | 15 | 30 | Kenya | ND | ND | |
| Tunisia | 15 | ND | Kosovo | ND | ND | |
| UAE | 20 | ND | Malaysia | ND | ND | |
| Germany | 30 | 30 | Mexico | ND | ND | |
| Malta | 30 | ND | Mozambique | ND | ND | |
| Ukraine | 30 | ND | Myanmar | ND | ND | |
| Estonia | 45 | ND | Netherlands | ND | ND | |
| Singapore | 45 | ND | New Zealand | ND | 20 | |
| Argentina | 60 | 60 | Norway | ND | ND | |
| Bulgaria | 60 | 60 | Panama | ND | ND | |
| Montenegro | 60 | 60 | Peru | ND | ND | |
| UK | 60 | 60 | Portugal | ND | ND | |
| UK – NI | 60 | 60 | Slovakia | ND | ND | |
| UK – Wales | 60 | 60 | Slovenia | ND | 10 | |
| China | 90 | ND | South Africa | ND | ND | |
| Paraguay | 180 | 180 | UK – Scotland | ND | ND | |
| Australia | ND | ND | Uruguay | ND | ND | |
| Austria | ND | ND | USA | ND | ND | |
| Belgium | ND | ND | Zimbabwe | ND | ND |
References
BAPD. 2020. BAPD urges government to reconsider PPE requirements for dentistry [Online]. Dentistry. [Accessed 30th July 2020 ].
BUONANNO, G., STABILE, L. & MORAWSKA, L. 2020. Estimation of airborne viral emission: Quanta emission rate of SARS-CoV-2 for infection risk assessment. Environ Int, 141, 105794.
CLARKSON J, RAMSAY C, RICHARDS D, ROBERTSON C, & ACEVES-MARTINS M; on behalf of the CoDER Working Group (2020). Aerosol Generating Procedures and their Mitigation in International Dental Guidance Documents – A Rapid Review.
CORNFORTH, D. M., MATTHEWS, A., BROWN, S. P. & RAYMOND, B. 2015. Bacterial Cooperation Causes Systematic Errors in Pathogen Risk Assessment due to the Failure of the Independent Action Hypothesis. PLoS Pathog, 11, e1004775.
FGDP. 2020. Implications of COVID-19 for the safe management of general dental practice A practical guide [Online]. [Accessed 30th July 2020 ].
HEFFERNAN, M. 2020. Is a one hour fallow period really necessary for dentistry in England? [Online]. Dentistry. [Accessed 30th July 2020 ].
HILL, I. 1987. 95% Confidence limits for the median. Journal of Statistical Computation and Simulation, 28, 80-81.
HOTA, B., STEIN, B., LIN, M., TOMICH, A., SEGRETI, J. & WEINSTEIN, R. A. 2020. Estimate of airborne transmission of SARS-CoV-2 using real time tracking of health care workers.
MORAWSKA, L. & MILTON, D. K. 2020. It is time to address airborne transmission of COVID-19. Clin Infect Dis, 6,ciaa939.
STADNYTSKYI, V., BAX, C. E., BAX, A. & ANFINRUD, P. 2020. The airborne lifetime of small speech droplets and their potential importance in SARS-CoV-2 transmission. Proc Natl Acad Sci U S A, 117, 11875-11877.
TALEB, N., READ, R. & DOUADY, R. 2020. The Precautionary Principle (with Application to the Genetic Modification of Organisms).
WHO 2020a. Modes of transmission of virus causing COVID-19: implications for IPC precaution recommendations: scientific brief, 27 March 2020. World Health Organization.
WHO 2020b. Transmission of SARS-CoV-2: implications for infection prevention precautions 9th July. World Health Organization.
ZWART, M. P., HEMERIK, L., CORY, J. S., DE VISSER, J. A., BIANCHI, F. J., VAN OERS, M. M., VLAK, J. M., HOEKSTRA, R. F. & VAN DER WERF, W. 2009. An experimental test of the independent action hypothesis in virus-insect pathosystems. Proc Biol Sci, 276, 2233-42.
Picture Credits
By Raghu deep darisi – Own work, CC BY-SA 4.0, Link
